
CASE REPORT
A 12-year-old boy presented for a routine ophthalmic examination. The patient was asymptomatic on presentation. His past ocular history was significant for bilateral congenital cataracts which required bilateral cataract extraction by phacoemulsification with posterior chamber intraocular lens (PCIOL) implantation at 2 months of age.

There was no other relevant medical (topical or systemic medication) or surgical history. Despite this intervention, the patient developed bilateral amblyopia and had severe nystagmus when either eye was occluded.
At the time of the presentation, his visual acuity was hand motion in both eyes. Tonometry and specular microscopy were not possible given the degree of nystagmus.
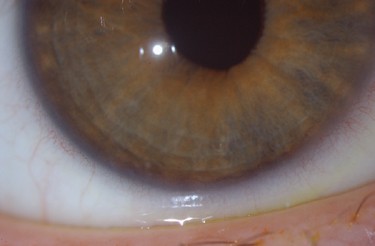
A slit lamp examination of the right eye revealed a clear cornea with a fine pigmented line involving 360 degrees of the peripheral endothelium and a clear PCIOL.
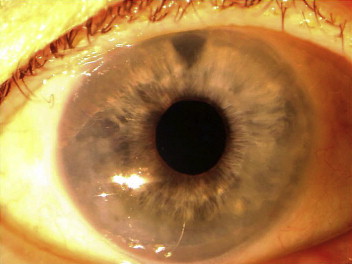
The left eye revealed normal conjunctiva, a clear central cornea with 360 degrees of peripheral stromal corneal edema with microbullae without epithelial defect, or vascularization, and a clear PCIOL.
The rest of the ocular examination was normal. These findings were consistent with incipient Brown McLean Syndrome (BMS) in the right eye and established BMS in the left eye. The patient remained asymptomatic, and no further treatment was started at the time.
Brown McLean Syndrome disease entity
Brown-McLean Syndrome (BMS) describes a condition in which the peripheral (2-3mm) inferior cornea becomes edematous and progresses circumferentially, sparing the central cornea in most cases.
First described in 1969 as “peripheral corneal edema after cataract extraction,” it was later renamed to Brown-McLean syndrome.
Although it was initially believed to be associated with underlying endothelial dystrophy, further supported by a possible genetic predisposition as some cases of relatives presenting with this condition have been identified, no causative dystrophy or gene has been identified.
While its pathophysiology is still unknown, it was initially described in aphakic patients classically after intracapsular lens extraction. Most patients were elderly although patients as young as 12 years old have been reported.
It typically occurs several years after surgery, averaging 6-16 years post-operative. Some speculations that a genetic predisposition for endothelial disease coupled with endothelial trauma has been proposed.
Other surgeries have been associated with BMS including include PK, anterior chamber intraocular lens (ACIOL), phacoemulsification, and pars plane vitrectomy with lensectomy.
Interestingly, endothelial trauma is not necessary to induce Brown-McLean syndrome. Ultrasound biomicroscopy does not always reveal the presence of iridocorneal apposition and the presence of an iridectomy is not always reported as protective.
Non-surgical cases of BMS include patients who have had lens subluxation, spontaneous lens resorption, endothelitis, keratoconus, angle closure glaucoma, or myotonic dystrophy.

Brown McLean Syndrome management
Medical therapy
Most cases of Brown-McLean syndrome are responsive to hypertonic saline and topical steroids. Patients can also trial contact lenses, which have been shown to be well tolerated despite peripheral corneal edema.
Surgical therapy
For refractory or symptomatic cases, surgical management may be warranted. In recurring cases of epithelial bullae secondary to Brown-McLean syndrome, an annular amniotic membrane transplant using two trephines of different diameters placed basement membrane side up has been shown to be successful while maintaining central visual acuity.
Anterior stromal puncture with a 23-G or 25-G needle can be used as well to induce collagen expression thereby improving epithelial cell adhesion and subepithelial fibrosis, both of which improve blockade of fluid penetration into the corneal epithelium.
In the cases of ACIOL–associated BMS, treatment often includes the removal of the ACIOL for the resolution of the corneal edema. In untreated cases where central corneal decompensation occurs, a corneal transplant may be necessary.
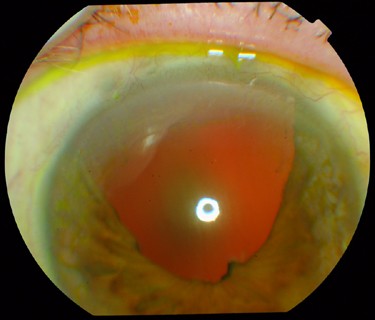
HOW TO TAKE SLIT-LAMP EXAM IMAGES WITH A SMARTPHONE?
Smartphone slit-lamp photography is the new advancement in the field of science and technology in which photographs of the desired slit-lamp finding can be taken with smartphones using slit-lamp adapters.
Slit-lamp Smartphone photography
REFERENCES
- Brown, S., and McLean, J. Peripheral corneal edema after cataract extraction a new clinical entity. Tr Am Acad Ophth Otol. 1969; 79:465.
- Brown, S. Peripheral Corneal Edema After Cataract Extraction. AJO. 1970; 70: 326-328.
- Charlin, R. Peripheral corneal edema after cataract extraction. Am J Ophthalmol. 1985; 99:298-303.
- Gothard T., Hardten D., Lane S., et al. Clinical findings in Brown-McClean Syndrome. Am J Ophthalmol. 1993; 115:729-737.
- Vote, B., Grupcheva, C., Ormonde, S., McGhee C. In vivo confocal microstructural analysis and surgical management of Brown McLean syndrome associated with spontaneous crystalline lens luxation. J Cataract Refract Surg. 2003; 29: 614-618.

{kind=link}