
CASE REPORT
A 32-year-old male patient presented to the ophthalmology clinic with a complaint of a visible mass in his left eye. He had no other significant medical history and was not taking any medications.

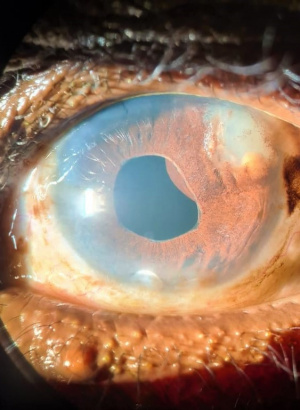
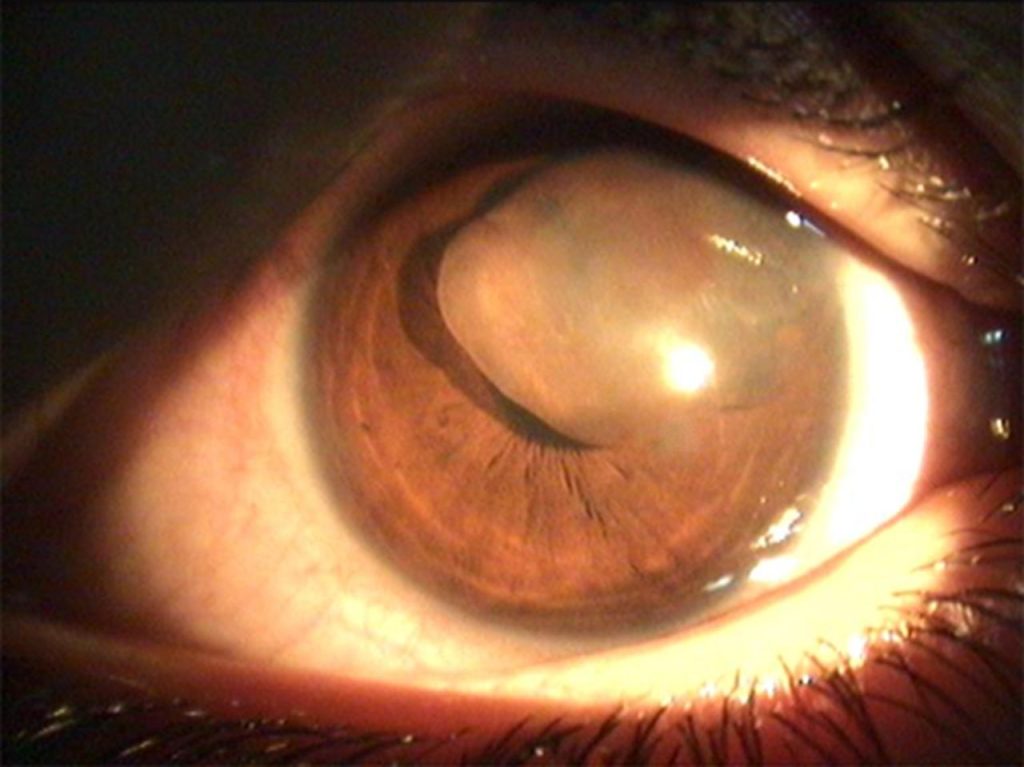
On examination, his visual acuity was 20/20 in both eyes. Slit-lamp examination revealed the presence of a round, well-defined cyst measuring approximately 3mm in diameter within the iris of his left eye. No other abnormalities were noted in the anterior or posterior segments of the eye.
Diagnostic imaging such as ultrasound biomicroscopy or ultrasound of the eye confirmed the diagnosis of an iris cyst. The patient was informed of the benign nature of the cyst and was advised to return for follow-up examinations to monitor for any changes in size or visual symptoms.
Iris Cysts DISEASE entity
Iris cyst is an epithelial-lined space that involves a layer of the iris. A primary iris cyst does not have a recognizable etiology. A secondary iris cyst has a recognizable etiology, such as surgical or nonsurgical trauma.

Primary iris cysts are congenital and occur sporadically. Iris pigment epithelium cysts occur more commonly in adults while iris stromal cysts occur more in children.
Primary iris cysts are nonkeratinized squamous epithelial-lined structures that arise either from the posterior iris layer or stroma. Epithelium from stromal cysts contains goblet cells.
The pathogenesis of primary iris cysts is not entirely understood, and proposed mechanisms in the literature are controversial. Iris pigment epithelial cysts are thought to be remnants of the marginal sinus of the iris that have not been obliterated.
The presence of goblet cells in iris stromal cysts suggests that they are formed by entrapped surface ectoderm tissue likely during the formation of the lens vesicle (4th week of embryogenesis).
Primary iris cysts are most commonly of posterior pigment epithelial cell origin and located in the peripheral iris.
MANAGEMENT of Iris Cysts
Medical treatment
Iris cysts secondary to miotics (phospholine iodide) are treated with phenylephrine 2.5%. Cysts also resolve with the discontinuation of phospholine iodide.
General treatment
Iris cysts that are stable and not causing symptoms or secondary complications require no treatment but should be followed regularly. Iris cysts that involve the visual axis, particularly in children at risk for amblyopia, necessitate intervention.
Most authors recommend treating iris cysts using a step-wise approach, starting with less-invasive treatment prior to proceeding to surgical excision whenever possible.
Surgery
- Laser Treatment
- Argon laser photocoagulation – photocoagulation of the cyst epithelium may be able to halt the production of cystic fluid contents. This may be performed to shrink the cysts; though recurrence is common. Its utility is limited in cases of large cysts and when visualization is difficult.
- Nd: YAG – photodisruption (laser cystostomy) of the cyst wall may allow perforation of the cyst and release of contents into the anterior chamber.
- Cyst aspiration with the injection of sclerosing agent– Aspiration of the cyst contents with subsequent injection of absolute alcohol to induce sclerosis and closure of the cystic cavity has demonstrated good success in a minimally-invasive method.
- Methods may vary, but a 27g infusion/aspiration needle can be used first to aspirate cyst contents, then infuse alcohol until the cyst wall turns grey, after which the alcohol is removed. While recurrence is not common, this procedure can be repeated if it does occur. Other sclerosing agents published in the literature include trichloroacetic acid, 5-fluorouracil, and mitomycin C.
- En bloc excision – A more aggressive surgical approach is the en bloc excision of the iris cyst with or without light cryotherapy. While this procedure has a good success rate, there is a greater risk of causing collateral damage to ocular structures.
- Secondary iris cysts due to epithelial downgrowth may require more aggressive surgical excision and devitalization of the epithelial tissues with vitrectomy, lensectomy, and cryodestruction of residual cells at the excision site.
HOW TO TAKE SLIT-LAMP EXAM IMAGES WITH A SMARTPHONE?
Smartphone slit-lamp photography is the new advancement in the field of science and technology in which photographs of the desired slit-lamp finding can be taken with smartphones by using the slit-lamp adapters.
Slit-lamp Smartphone photography
REFERENCES
- Shields JA. 1981. Primary cysts of the iris. Trans Am Ophthalmol Soc 79: 771-809.
- Shields JA, Kline MW & Ausberger JJ. 1984. Primary iris cysts: a review of the literature and report of 62 cases. Br J Ophthalmol 68: 152-166.
- Primary Iris Cysts. AAO Basic and Clinical Science Course Section 6: Pediatric Ophthalmology and Strabismus. Elsevier, 2013.
- Grutzmacher RD, Lindquist TD, Chittum ME, Bunt-Milam AH & Kalina RE. 1987. Congenital iris cysts. Br J Ophthalmol 71: 227-234.
- Naumann G & Green WR. 1967. Spontaneous nonpigmented iris cysts. Arch Ophthalmol 78: 496-500. doi: 10.1002/archopht.1967.00980030498016.
- Paridaens AD, Deuble K & McCartney AC. 1992. Spontaneous congenital non-pigmented epithelial cysts of the iris stroma. Br J Ophthalmol 76: 39-42.
- Shields CL, Kancherla S, Patel J, Vijayvargiya P, Suriano MM,Kolbus E, Badami A, Sharma P, Jacobs E, Voluck M, Zhang Z, Kansal R, Shields PW, Bianciotto CG & Shields JA. 2012. Clinically survey of 3680 iris tumors based on patient age at presentation. Ophthalmology 119: 407-414. doi: 10.1016/j.ophtha.2011.07.059.

{kind=link}