
CASE REPORT
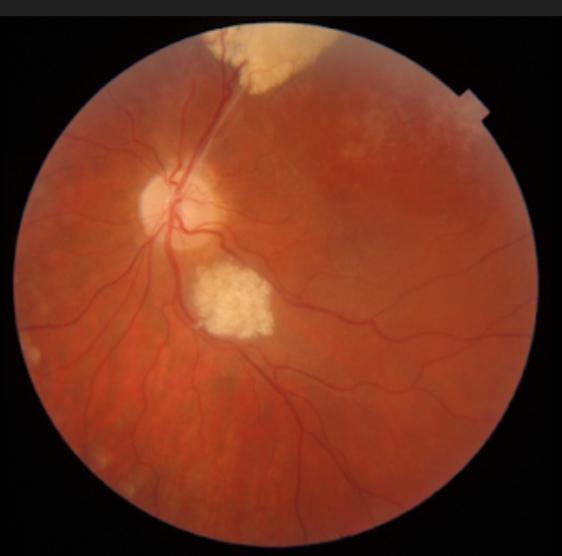
A 65-year-old female visited an eye clinic with a presenting complaint of decreased vision in her right eye. On testing Visual acuity, it was recorded as OD: 6/36, OS: 6/9. On a fundus examination, raised mulberry-like lesions were seen.

On OCT, subretinal fluid was also noticeable. This patient was treated with bevacizumab as the first treatment of choice and it resulted in significant improvement in her visual acuity. Genetic testing was done to rule out its leading Aetiology of either tuberous sclerosis complex, neurofibromatosis, or others but it was found negative.
Based on fundus findings and OCT report, the diagnosis was confirmed as a retinal astrocytic hamartoma.
Retinal astrocytic hamartoma entity
Retinal astrocytic hamartoma is a benign retinal tumor composed of astrocytic glial cells having frequent association with tuberous sclerosis complex(TSC) and rare association with neurofibromatosis.
Other associations are as follows:
- Retinitis pigmentosa (RP)
- Stargardt’s disease
- Gyrate atrophy
- Usher’s syndrome
In 1921, it was recognized first time by Van der Hoeve who named the lesions(tumors) “phakomas”.
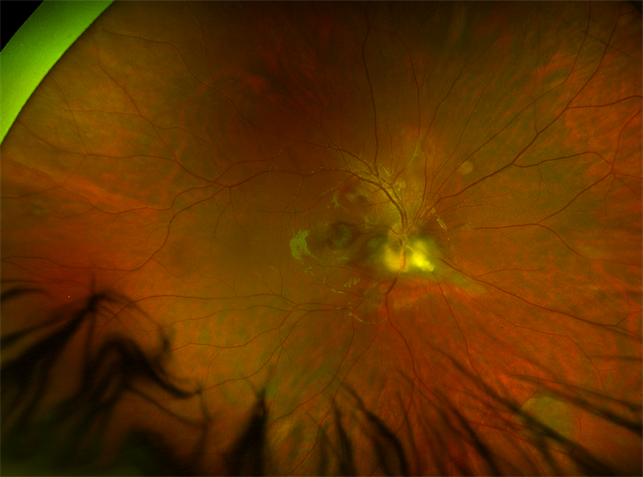
Retinal astrocytic hamartoma patients are usually asymptomatic but if lesions(tumors) are present in the macular or optic nerve region, it can lead to decreased vision, Metamorphopsia, or floaters. Fundus findings show raised multilobulated and well demarcated white yellow lesions in the peripheral retina.
Morphologically, retinal astrocytic hamartoma can be classified into 3 types.
Type 1:
In this type, non-calcified grey-white lesions are seen which are flat and smooth. It is the most commonly occurring type.
Type 2:
In this type, mulberry-like lesions are seen which are multinodular, raised, and calcified as well.
Type 3:
This type of retinal astrocytic hamartoma has mixed signs of both type 1 and type 2.
Diagnostic procedures
It can be misdiagnosed with retinoblastoma so a B scan and OCT help distinguish retinal astrocytic hamartoma from retinoblastoma
OCT:
Spectral-domain (SD) OCT is thought to be more effective in diagnosing RAH. It shows dome-shaped thickening of the inner retina and intralesional calcification in the form of empty spaces. The outer retina might be compressed or disorganized by the tumor.
Ultrasound:
It demonstrates the tumor as well as hyperechogenic calcifications.
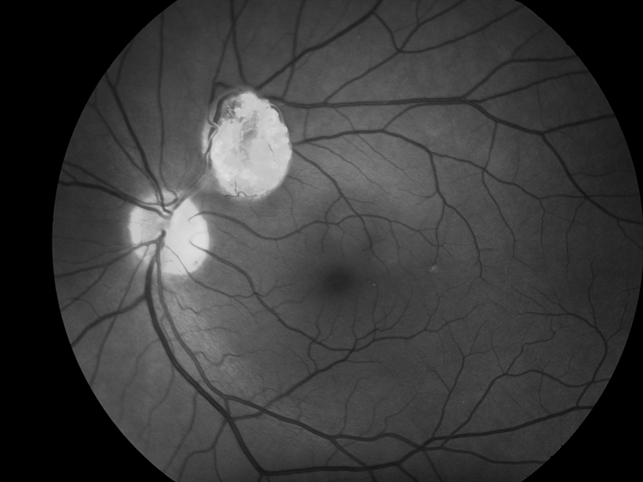
Fundus Autofluorescence(FAF):
It is done to differentiate between calcified and non-calcified tumors. Calcified tumors show hyper autofluorescence and non-calcified tumors show reduced autofluorescence.
Fluorescein Angiography:
It helps identify those tumors which are not visible clinically.
MANAGEMENT
Generally, retinal astrocytic hamartoma is treated early with anti-VEGF agents such as bevacizumab at frequent intervals. mTOR Inhibitors (sirolimus or everolimus) are usually used in patients with TSC.
In the case of aggressive RAH, other therapies can be used such as photodynamic therapy, laser photocoagulation, and Dexamethasone implant.

Would you have interest in taking retina images by smartphone?
Fundus photography is superior to fundus analysis as it enables intraocular pathologies to be photo-captured and encrypted information to be shared with colleagues and patients.
Recent technologies allow smartphone-based attachments and integrated lens adaptors to transform the smartphone into a portable fundus camera and Retinal imaging by smartphone.
RETINAL IMAGING BY YOUR SMARTPHONE
REFERENCES
- Amoroso F, Souied EH, Bruyère E, Astroz P, Mouallem-Beziere A, Pedinielli A, Miere A. Two-year follow-up of a retinal astrocytic hamartoma imaged by optical coherence tomography angiography. Retin Cases Brief Rep. 2020 Jan 29; doi: 10.1097/ICB.0000000000000975.
- Bennett LW. Isolated retinal astrocytic hamartoma. Clin Exp Optom. 2020 May;103(3):382–383. doi: 10.1111/cxo.12956.
- Zhang P, Sun D, Zhu J, Li J, Wang Y. Image features of retinal astrocytic hamartoma in a patient with tuberous sclerosis complex. Eye Sci. 2014 Dec;29(4):223–226.
- Shields JA, Shields CL. Glial tumors of the retina and optic disc. In: Shields JA, Shields CL, editors. Intraocular tumors. A Text and Atlas. Philadelphia: WB Saunders; 2008. pp. 405–27.
- Nyboer JH, Robertson DM, Gomer MR. Retinal lesions in tuberous sclerosis. Arch Ophthalmol. 1976;94:1277–80.
- Crino P, Nathanson K, Henske E. The tuberous sclerosis complex. N Engl J Med. 2006;355:1345–56.

{kind=link}