
CASE REPORT
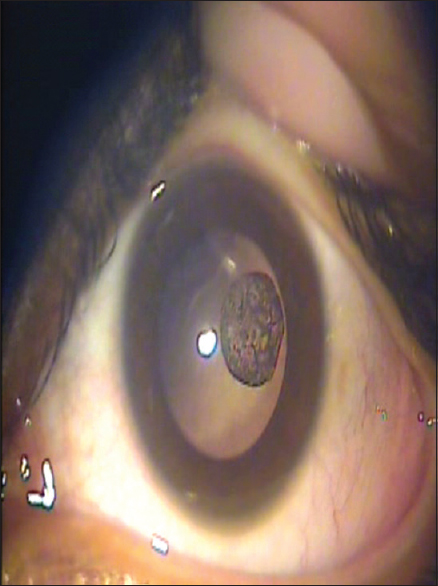
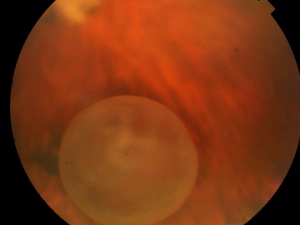
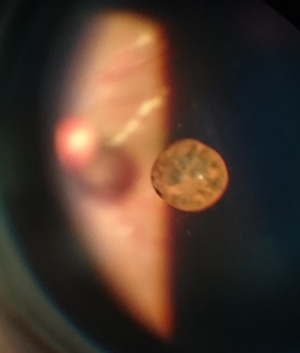
Intraocular pressure was 18 and 16 mmHg in his right and left eye, respectively, with Goldmann applanation tonometer. After dilation, the right eye showed 6 mm × 4 mm of solitary pigmented freely floating cyst in the vitreous.
Indirect ophthalmoscopy and posterior segment biomicroscopy performed with a 90 D lens were unremarkable in the left eye, but a single, oval 6 mm × 4 mm diameter cyst was identified in the right eye, floating freely in the vitreous.
The cyst was partially masking the underlying retinal vasculature. B-scan ultrasonography showed an echo-free, round-shaped cyst that was free from surrounding vitreous strands or retina. Optical coherence tomography was normal in both eyes.
Serology was negative for indirect hemagglutination tests of the patient for Echinococcus and cysticercosis. Eosinophilia was not detected in the peripheral blood smear. Casoni skin test was negative. Based on these findings, the patient was diagnosed as primary vitreous cyst.
Vitreous cysts entity
Vitreous cysts are rare clinical entities that can occur in a normal eye or in an eye associated with other pathologies.

- Floating vitreous cysts are extremely rare clinical entities that are regarded as ‘ocular curiosities’.
- They can either be an incidental finding in a normal eye or associated with other ocular pathologies.
- It was first described by Tansley in 1899 as an irregular spherical cyst that showed lines of pigment on its surface.
Vitreous cysts can be congenital or acquired.
Congenital Cysts
- Remnants of the hyaloid vascular system.
- Located at the hyaloid canal and found in conjunction with a Mittendorf’s dot or Bergmeister’s papillae.
- They are usually stable, do not progress, and rarely interfere with visual acuity.
- They are usually non-pigmented pearl-gray cysts with smooth surfaces and can be sessile or pedunculated.
- They are located anterior to the optic disc.
- Some can be limited in movement due to vitreous strands attaching the cyst to the optic disc.
Acquired Cysts
- They have been reported to occur secondary to or associated with:
- Ocular trauma.
- Intraocular inflammation/infection/ uveitis eg. Intermediate Uveitis, Toxoplasmosis.
- Retinal diseases such as Retinitis pigmentosa, Choroidal atrophy, Retinoschisis, High myopia with uveal coloboma, etc.
- Retinal detachment surgeries
- They are usually symptomatic and associated with a reduction in visual acuity.
Types
Pigmented Cysts
- Likely originate from the pigment epithelium of the iris or ciliary body and later become detached into the vitreous.
- They are brown in color.
Non-Pigmented Cysts
- Congenital cysts are usually non-pigmented and originate from the hyaloidal vascular system.
- They are translucent, mobile, and yellow-gray in color.
MANAGEMENT of Vitreous Cysts
Asymptomatic cysts
- Observation and follow-up
Symptomatic cysts
- Laser cystotomy by Argon laser or Nd:Yag laser.
- Pars plana vitrectomy with cyst excision.
Would you have interest in taking retina images by smartphone?
Fundus photography is superior to fundus analysis as it enables intraocular pathologies to be photo-captured and encrypted information to be shared with colleagues and patients.
Recent technologies allow smartphone-based attachments and integrated lens adaptors to transform the smartphone into a portable fundus camera and Retinal imaging by smartphone.
RETINAL IMAGING BY YOUR SMARTPHONE
REFERENCES
- Duke-Elder S. System of Ophthalmology. Vol. 3. Normal and Abnormal Development. Part 2.Congenital Deformities. London: Henry Kimpton, 1964:763
- Tansley JO. “Cyst of the vitreous”. Transactions of the American Ophthalmological Society 8 (1899): 507-509.
- Bullock JD. Developmental vitreous cysts. Arch Ophthal. 1974;91:83–84.
- Pannarale C. On a case of preretinal mobile cysts in a subject affected by congenital toxoplasmosis (in Italian) G Ital Oftalmol. 1964;17:306–317.
- Tranos PG, Ferrante P, Pavesio C. Posterior vitreous cyst and intermediate uveitis. Eye. 2010;24:1115–1116.
- Tuncer S, Bayramoglu S. Pigmented free-floating vitreous cyst in a patient with high myopia and uveal coloboma simulating choroidal melanoma. Ophthalmic Surg Lasers Imaging. 2011;42(Online):e49–e52.

{kind=link}