
Introduction
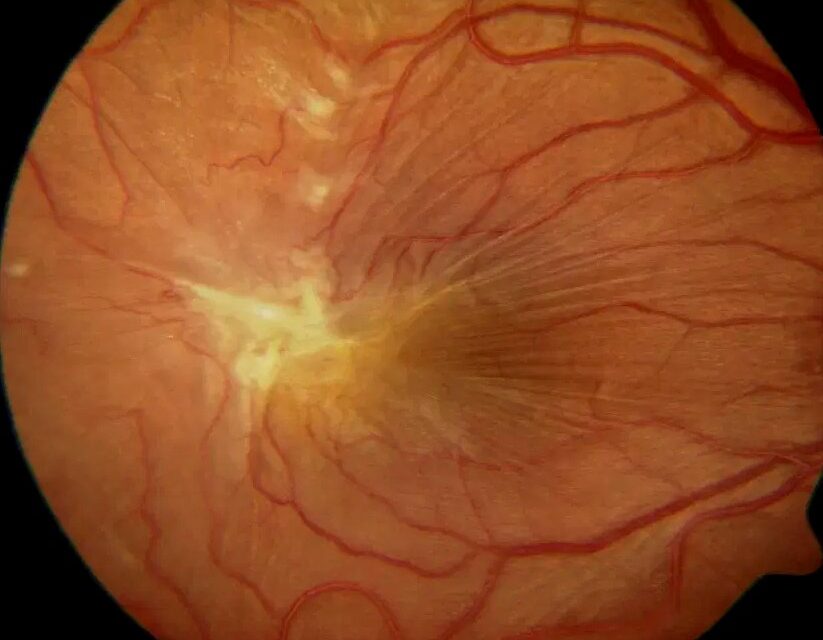
Epiretinal membrane (ERM), also known as macular pucker, is a common vitreoretinal condition characterized by the proliferation of fibrocellular tissue on the inner retinal surface.

While many ERMs remain stable and require only observation, symptomatic cases can cause decreased visual acuity, metamorphopsia, micropsia, and impaired quality of life.
Pars plana vitrectomy with membrane peeling has become the standard surgical treatment for visually significant ERM, often resulting in substantial anatomical and functional improvement.
However, despite successful surgery, some patients experience recurrence of the membrane, leading to renewed retinal distortion and visual symptoms.
Although recurrence rates are generally low, understanding why ERMs recur and how recurrence can be minimized remains important for retina specialists aiming to achieve durable long-term outcomes.
What Is Epiretinal Membrane Recurrence?
ERM recurrence refers to the reappearance of fibrocellular proliferation on the retinal surface following surgical removal of the original membrane.
Recurrence may manifest as:
- A new membrane develops after complete removal
- Regrowth of residual membrane tissue
- Progressive retinal wrinkling after initial improvement
- Reappearance of visual symptoms
Not all recurrent membranes become clinically significant. Some remain mild and asymptomatic, while others may require repeat surgery.
👉 Anatomical recurrence does not always translate into functional recurrence.
How Common Is ERM Recurrence?
Reported recurrence rates vary depending on:
- Duration of follow-up
- Surgical technique
- Use of internal limiting membrane (ILM) peeling
- Underlying retinal pathology
Studies have reported recurrence rates ranging from:
- Approximately 5% to 20%
Clinically significant recurrence requiring reoperation is considerably less common.
Modern surgical techniques have reduced recurrence rates substantially compared with earlier approaches.
Why Do Epiretinal Membranes Recur?
Recurrence typically occurs because cellular proliferation continues or restarts after surgery.
The retinal surface remains biologically active, and several cell types can contribute to membrane formation, including:
- Müller cells
- Retinal pigment epithelial cells
- Fibroblasts
- Myofibroblasts
- Inflammatory cells
Even after apparently complete removal, microscopic residual cells may remain capable of proliferation.
Major Risk Factors for ERM Recurrence
1. Absence of Internal Limiting Membrane Peeling
One of the strongest predictors of recurrence is failure to remove the internal limiting membrane.
Why the ILM Matters
The ILM serves as a scaffold for cellular proliferation.
If left intact:
- Residual cells may migrate and proliferate
- New membrane formation becomes more likely
- Tangential traction may redevelop
Numerous studies have demonstrated significantly lower recurrence rates when ILM peeling accompanies ERM removal.
👉 ILM peeling is widely considered one of the most effective strategies for reducing recurrence.
2. Incomplete Membrane Removal
Microscopic residual membrane fragments may remain attached to the retinal surface.
These remnants can serve as a source for:
- Continued cellular proliferation
- Progressive membrane regrowth
- Recurrent traction
High-magnification visualization and intraoperative staining help improve completeness of removal.
3. Secondary Epiretinal Membranes
Secondary ERMs tend to recur more frequently than idiopathic ERMs.
Common causes include:
- Retinal detachment
- Retinal tears
- Diabetic retinopathy
- Retinal vein occlusion
- Ocular inflammation
- Ocular trauma
These conditions provide ongoing stimuli for cellular proliferation.
👉 Secondary ERMs often behave more aggressively than idiopathic membranes.
4. Younger Age
Several studies have suggested that younger patients may have higher recurrence rates.
Possible explanations include:
- Greater cellular activity
- Stronger wound-healing response
- Increased proliferative potential
Although recurrence remains uncommon overall, younger individuals may require closer follow-up.
5. Ongoing Inflammation
Inflammatory mediators play an important role in membrane formation.
Conditions associated with chronic inflammation include:
- Uveitis
- Diabetic retinopathy
- Postsurgical inflammation
- Chronic retinal vascular disease
Persistent inflammation may promote recurrent fibrocellular proliferation.
6. Proliferative Vitreoretinopathy-Like Changes
Some recurrent ERMs exhibit features resembling mild proliferative vitreoretinopathy (PVR).
These cases may demonstrate:
- Increased contractility
- More aggressive membrane growth
- Greater retinal distortion
Such membranes are often more challenging to manage surgically.
The Role of Internal Limiting Membrane Peeling
The debate regarding ILM peeling has largely shifted in favor of routine use during ERM surgery.
Benefits Include
- Lower recurrence rates
- Removal of cellular scaffolding
- Reduced tangential traction
- Improved anatomical stability
Potential Concerns
- Mechanical trauma to the inner retinal layers
- Dissociated optic nerve fiber layer appearance
- Rare microstructural retinal changes
Despite these concerns, the recurrence-reduction benefits generally outweigh the risks in most cases.
👉 Today, many retina surgeons routinely combine ERM and ILM peeling during primary surgery.
OCT Findings Suggestive of Recurrence
Optical coherence tomography remains the most important tool for postoperative monitoring.
Early Signs Include
- Surface wrinkling of the retina
- Progressive retinal thickening
- Reappearance of tractional changes
- Distortion of the foveal contour
Advanced Findings
- Significant retinal folds
- Increased central retinal thickness
- Recurrent macular edema
- Loss of foveal architecture
Serial OCT imaging often detects recurrence before symptoms become significant.
Clinical Symptoms of Recurrent ERM
Patients may report:
- Gradual visual decline
- Recurrent metamorphopsia
- Image distortion
- Difficulty reading
- Reduced contrast sensitivity
However, some recurrent membranes remain asymptomatic and are discovered during routine follow-up examinations.
Does Recurrence Always Require Surgery?
No.
Management depends on:
- Visual acuity
- Symptom severity
- Degree of retinal distortion
- Patient expectations
Many recurrent membranes can be observed safely.
Indications for Repeat Surgery
- Significant visual deterioration
- Progressive metamorphopsia
- Marked OCT evidence of traction
- Functional impairment affecting daily activities
👉 Surgical decisions should be guided by symptoms and retinal function, not OCT appearance alone.
Prevention Strategies
1. Thorough Primary Surgery
Key surgical principles include:
- Complete ERM removal
- Careful inspection of the retinal surface
- Adequate vitreous removal
Meticulous technique reduces residual proliferative tissue.
2. Routine ILM Peeling
Perhaps the most effective preventive strategy.
Benefits include:
- Reduced recurrence risk
- Improved long-term stability
- Elimination of cellular scaffolds
3. Use of Vital Dyes
Dyes improve the visualization of transparent tissues.
Commonly used agents include:
- Brilliant Blue G
- Trypan Blue
- Dual staining techniques
Better visualization improves the completeness of peeling.
4. Control Underlying Disease
When secondary ERMs are present, treatment should also target the underlying pathology.
Examples include:
- Diabetic retinopathy management
- Uveitis control
- Retinal vascular disease treatment
Failure to address the underlying cause may promote recurrence.
5. Long-Term OCT Surveillance
Regular follow-up allows early detection of:
- Recurrent membrane formation
- Macular edema
- Progressive traction
Early recognition facilitates timely intervention when necessary.
Future Perspectives
Advances in vitreoretinal surgery continue to improve outcomes.
Emerging areas of research include:
- Pharmacologic inhibition of cellular proliferation
- Anti-fibrotic therapies
- Improved intraoperative imaging
- Enhanced retinal staining techniques
- Molecular biomarkers predicting recurrence
These developments may further reduce recurrence rates in the future.
References
- Pesin SR, et al. “Vitrectomy for premacular fibroplasia: prognostic factors, long-term follow-up, and time course of visual improvement.” Ophthalmology. 1991.
- Park DW, et al. “Macular pucker removal with and without internal limiting membrane peeling.” Ophthalmology. 2003.
- Kwok AKH, et al. “Indocyanine green-assisted internal limiting membrane removal in epiretinal membrane surgery.” Ophthalmology. 2004.
- Azzolini C, et al. “Epiretinal membrane recurrence after surgical removal.” Graefes Arch Clin Exp Ophthalmol. 2017.
- Chang WC, et al. “Recurrence of epiretinal membrane after surgery.” Retina. 2013.
- Steel DHW, Lotery AJ. “Idiopathic epiretinal membrane management and outcomes.” Eye (Lond). 2013.

RETINAL IMAGING BY YOUR SMARTPHONE
{kind=link}