

Case Study
A male infant born at 27 weeks of gestation with a birth weight of 900 grams was admitted to the neonatal intensive care unit for respiratory distress syndrome.

Prolonged supplemental oxygen therapy was required during the first weeks of life. At 3 months of corrected age, ophthalmic screening revealed leukocoria and poor fixation in both eyes.
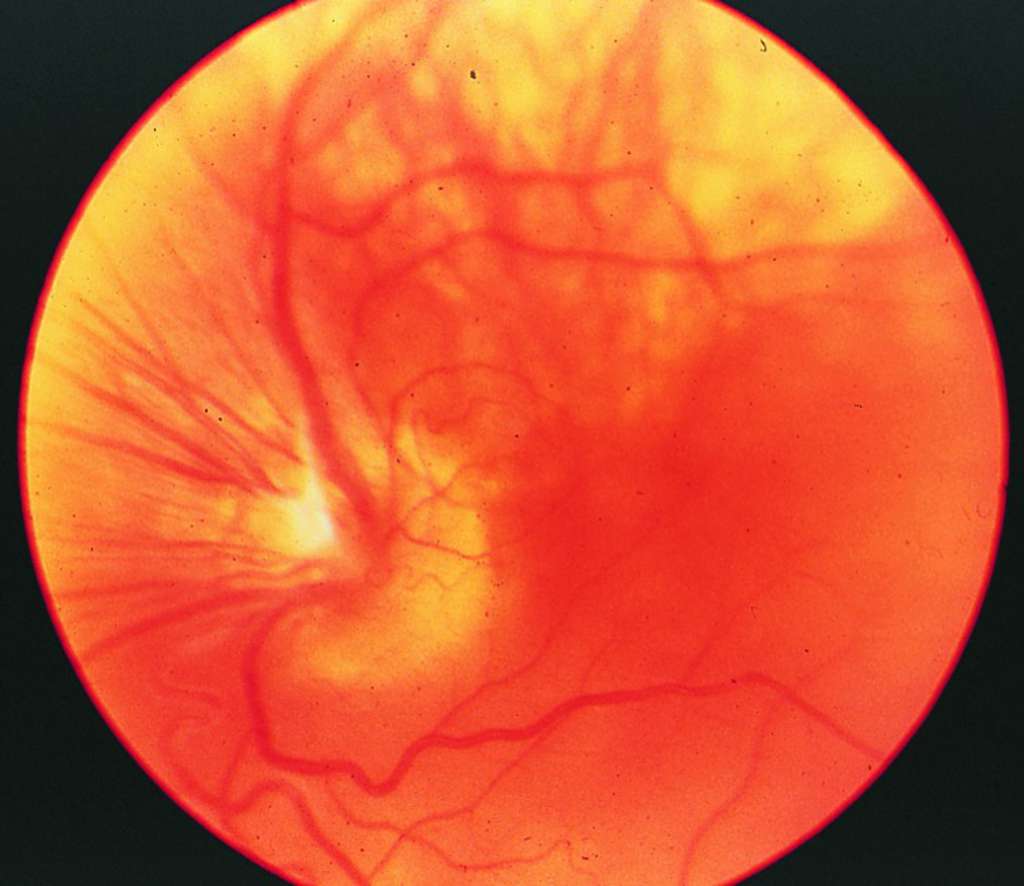
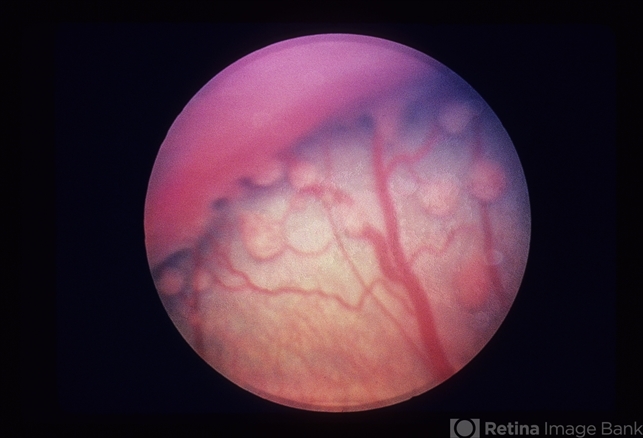
Fundus examination showed dense fibrovascular tissue behind the lens with tractional retinal detachment. A diagnosis of retrolental fibroplasia was made.
Disease Entity
Retrolental fibroplasia (RLF) is a historical term describing a severe, blinding retinal disorder observed in premature infants exposed to high concentrations of supplemental oxygen.
The disease is now recognized as the most advanced form of retinopathy of prematurity (ROP).
Although classic RLF is rare in modern practice, its historical significance has shaped neonatal care and ophthalmic screening protocols worldwide.
The condition is characterized by abnormal retinal vascular development leading to fibrovascular proliferation, tractional retinal detachment, and the formation of a fibrous membrane posterior to the crystalline lens.
Historical Perspective
RLF emerged as a major cause of childhood blindness in the 1940s and 1950s, coinciding with widespread, unregulated use of high-flow oxygen in neonatal care.
The link between oxygen exposure and retinal vascular damage was later established, leading to dramatic changes in neonatal oxygen management.
These discoveries marked one of the earliest examples of iatrogenic disease prevention through evidence-based practice.
Pathophysiology
Normal retinal vascularization proceeds from the optic disc toward the periphery during late gestation. In premature infants, this process is incomplete at birth.
Exposure to high oxygen levels suppresses vascular endothelial growth factor (VEGF), causing vaso-obliteration of immature retinal vessels.
Subsequent relative hypoxia after oxygen withdrawal stimulates excessive VEGF production, leading to:
-
Pathologic neovascularization
-
Fibrovascular proliferation
-
Vitreoretinal traction
-
Retinal detachment
In advanced stages, this fibrovascular tissue contracts, pulling the retina anteriorly and forming a dense retrolental membrane.
Epidemiology
Classic retrolental fibroplasia is now rare in developed healthcare systems due to improved neonatal practices.
However, severe ROP remains a significant concern worldwide, particularly in regions with limited access to controlled oxygen delivery and systematic screening programs.
Risk factors include:
-
Extreme prematurity
-
Low birth weight
-
Prolonged or unmonitored oxygen therapy
-
Systemic illness and sepsis
Clinical Features
Infants with advanced disease may present with:
-
Leukocoria
-
Absent or poor red reflex
-
Poor visual fixation
-
Nystagmus
-
Microphthalmia in chronic cases
Early stages are typically asymptomatic, highlighting the importance of routine screening.
Examination Findings
Ophthalmic examination may reveal:
-
Peripheral avascular retina
-
Ridge formation at the junction of vascular and avascular retina
-
Neovascularization and fibrovascular proliferation
-
Tractional or total retinal detachment
-
Fibrous retrolental membrane in end-stage disease
Indirect ophthalmoscopy and wide-field retinal imaging are essential for accurate assessment.
Differential Diagnosis
Conditions that may mimic retrolental fibroplasia include:
-
Persistent fetal vasculature
-
Congenital cataract
-
Retinoblastoma
-
Coats disease
Careful history and examination are required to differentiate these entities.
Diagnosis
Diagnosis is based on:
-
Gestational age and birth history
-
Retinal findings consistent with advanced ROP
-
Staging and zoning according to the international ROP classification
Ancillary imaging may assist in documentation and follow-up.
Management
Prevention
-
Strict regulation of oxygen therapy
-
Continuous oxygen saturation monitoring
-
Universal ROP screening programs
Treatment
-
Peripheral retinal ablation using laser photocoagulation
-
Intravitreal anti-VEGF therapy in selected cases
-
Vitreoretinal surgery for advanced tractional detachments
Early intervention significantly improves outcomes.

Prognosis
Visual prognosis depends on disease severity and timing of intervention. Advanced RLF carries a poor prognosis, with many patients developing profound visual impairment.
Modern preventive strategies have dramatically reduced the incidence of blinding disease.
Would you have interest in taking retinal images with your smartphone?
Fundus photography is superior to fundus analysis as it enables intraocular pathologies to be photo-captured and encrypted information to be shared with colleagues and patients.
Recent technologies allow smartphone-based attachments and integrated lens adaptors to transform the smartphone into a portable fundus camera and Retinal imaging by smartphone.
RETINAL IMAGING BY YOUR SMARTPHONE
References
-
Terry TL. Extreme prematurity and fibroblastic overgrowth of persistent vascular sheath behind each crystalline lens. Am J Ophthalmol.
-
Gilbert C, Foster A. Childhood blindness in the context of VISION 2020. Bull World Health Organ.
-
American Academy of Ophthalmology. Basic and Clinical Science Course: Retina and Vitreous.
-
Good WV. Retinopathy of prematurity: past, present, and future. Arch Ophthalmol.
-
Smith LEH. Pathogenesis of retinopathy of prematurity. Semin Neonatol.

{kind=link}