

Case Study
A 26-year-old male presented to the ophthalmology clinic complaining of mild blurred vision in his right eye following a blunt ocular trauma sustained during a sports accident six months earlier.


He reported no ocular pain, redness, or photophobia. His past ocular history was unremarkable. On examination, best-corrected visual acuity was 20/25 in the affected eye and 20/20 in the fellow eye.
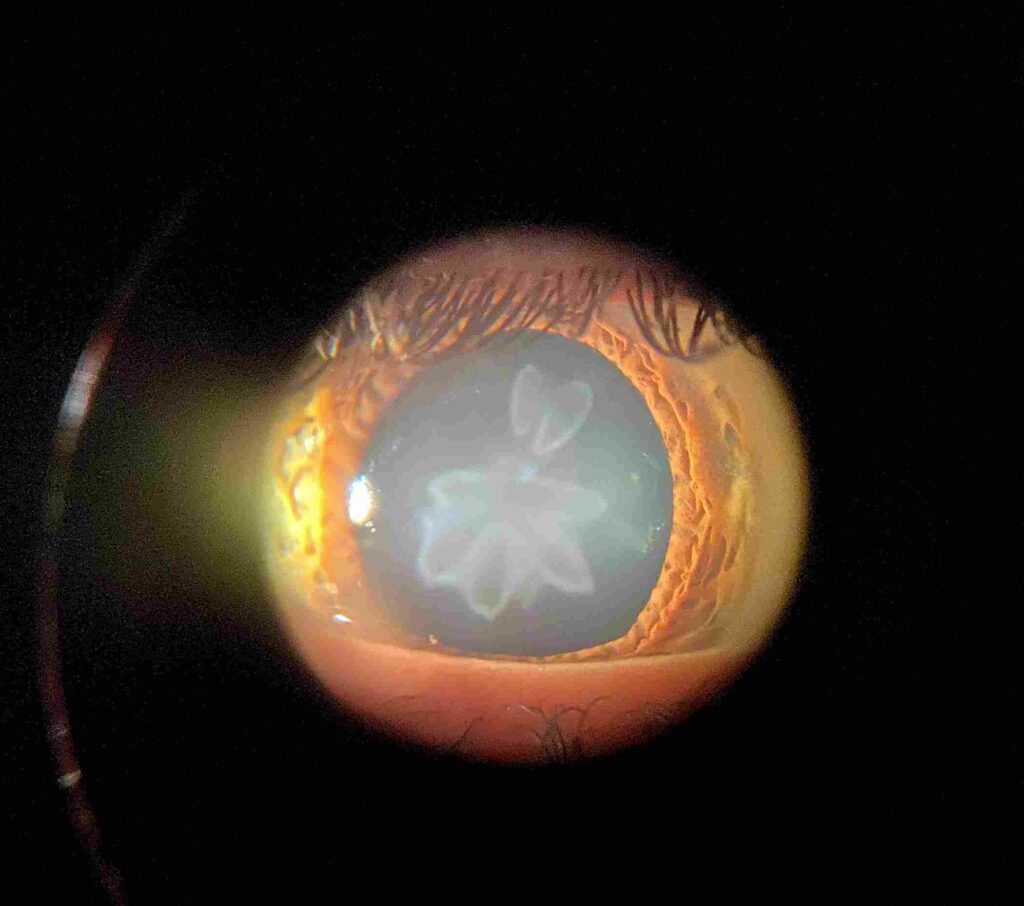
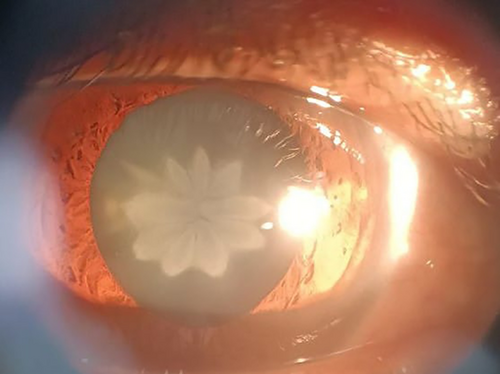
Slit-lamp examination revealed a characteristic star- or flower-shaped opacity located in the posterior cortex of the crystalline lens, with otherwise clear lens zones.
The anterior segment and fundus examination were normal. Based on the clinical appearance and trauma history, a diagnosis of rosette-shaped cataract was made.
Disease Entity
Rosette-shaped cataract is a distinctive form of traumatic cataract characterized by a stellate or petaloid opacity within the lens, most commonly involving the posterior cortical or posterior subcapsular region.
The term “rosette” refers to the flower-like configuration of lens opacification, which is highly suggestive of previous blunt ocular trauma.
Although classically associated with trauma, rosette-shaped cataracts may also occur in non-traumatic settings, including electrical injury, radiation exposure, or metabolic disturbances.
Recognition of this pattern is clinically important, as it often provides a historical clue to prior ocular insult, even when the patient does not recall a significant injury.
Pathophysiology
The development of a rosette-shaped cataract is primarily related to shock wave transmission through the globe following blunt trauma.
When an external force impacts the eye, mechanical energy is transmitted posteriorly, leading to focal disruption of lens fibers.
Key mechanisms include:
-
Sudden deformation of the globe, causing equatorial expansion
-
Disruption of posterior cortical lens fibers
-
Localized lens protein denaturation
-
Altered lens metabolism and hydration
The posterior cortex is particularly vulnerable due to its proximity to the vitreous body, which efficiently transmits concussive forces.
Over time, these focal changes coalesce into the characteristic stellate or rosette configuration.
Etiology
Common causes of rosette-shaped cataract include:
-
Blunt ocular trauma (most common)
-
Sports-related eye injuries
-
Motor vehicle accidents
-
Electrical injuries
-
Ionizing radiation exposure
-
Rare metabolic or toxic insults
In some cases, the cataract may develop months or even years after the inciting event, leading to delayed presentation.
Epidemiology
Rosette-shaped cataracts are most frequently observed in:
-
Young adults and adolescents
-
Male patients, reflecting higher exposure to trauma
-
Individuals with occupational or sports-related risk
There is no genetic predisposition, and the condition is typically unilateral, corresponding to the site of injury.
Clinical Features
Patients may be asymptomatic or present with mild visual disturbances, depending on the size and location of the opacity.
Common symptoms include:
-
Blurred or hazy vision
-
Glare, especially in bright light
-
Reduced contrast sensitivity
-
Minimal progression in many cases
Notably, visual acuity may remain relatively preserved if the central visual axis is spared.
Examination Findings
Slit-Lamp Examination
-
Stellate, star-shaped, or flower-like lens opacity
-
Usually located in the posterior cortex or posterior subcapsular region
-
Clear surrounding lens fibers in the early stages
-
No associated anterior segment inflammation
Dilated Examination
-
The fundus is typically normal unless associated trauma caused posterior segment injury
Imaging
-
Anterior segment OCT may help localize lens involvement
-
Ultrasound is reserved for cases with poor fundus view or suspected posterior pathology
Differential Diagnosis
Conditions that may mimic or be confused with rosette-shaped cataract include:
-
Posterior subcapsular cataract
-
Congenital lamellar cataract
-
Radiation-induced cataract
-
Electric cataract
-
Metabolic cataracts
A history of trauma and the characteristic morphology help distinguish rosette cataracts from other lens opacities.
Diagnosis
Diagnosis is primarily clinical, based on:
-
Characteristic rosette or stellate lens opacity
-
History of blunt trauma or ocular insult
-
Absence of inflammatory or degenerative signs
No laboratory testing is required. Careful documentation of lens morphology is essential for follow-up and surgical planning if needed.
Management
Management depends on symptom severity and visual impact.
Observation
-
Indicated for mild cases with minimal visual disturbance
-
Regular follow-up to monitor progression
-
Patient education regarding symptoms of worsening vision
Surgical Management
-
Cataract extraction is indicated when visual acuity becomes functionally limiting
-
Standard phacoemulsification is usually effective
-
Surgeons should assess for associated zonular weakness or capsular compromise in traumatic cases
In most patients, surgical outcomes are excellent.
Prognosis
The prognosis of rosette-shaped cataract is generally favorable.
-
Many cases remain stable for long periods
-
Visual prognosis after surgery is excellent if no associated ocular damage exists
-
Prognosis depends largely on the presence or absence of concurrent traumatic injuries such as retinal tears, macular damage, or angle recession
Prevention
Preventive strategies focus on:
-
Use of protective eyewear during sports and high-risk occupations
-
Early ophthalmic evaluation following ocular trauma
-
Patient education regarding delayed visual symptoms after injury
HOW TO TAKE SLIT-LAMP EXAM IMAGES WITH A SMARTPHONE?
Smartphone slit-lamp photography is the new advancement in the field of science and technology, in which photographs of the desired slit-lamp finding can be taken with smartphones by using the slit-lamp adapters.
Slit-lamp Smartphone photography
References
-
Kanski JJ, Bowling B. Clinical Ophthalmology: A Systematic Approach. 9th ed. Elsevier.
-
Yanoff M, Duker JS. Ophthalmology. 5th ed. Elsevier.
-
Tasman W, Jaeger EA. Duane’s Ophthalmology. Lippincott Williams & Wilkins.
-
Duke-Elder S. System of Ophthalmology. Vol. XI. Henry Kimpton.
-
American Academy of Ophthalmology. Basic and Clinical Science Course: Lens and Cataract

{kind=link}