
Case Presentation
A 42-year-old woman presented with progressive bilateral drooping of the eyelids and difficulty moving her eyes over the past five years.

She reported no pain, diplopia, or visual loss but noted reliance on head movements to track objects.
Her medical history included mild sensorineural hearing loss diagnosed in her thirties and proximal limb weakness without dysphagia or cardiac symptoms.
Family history revealed similar ptosis in her mother. Examination showed severe bilateral ptosis with marginal reflex distance of 1 mm, complete absence of upgaze and downgaze, restricted horizontal ductions to 10 degrees, normal pupil reactivity, and compensatory frontalis overaction.
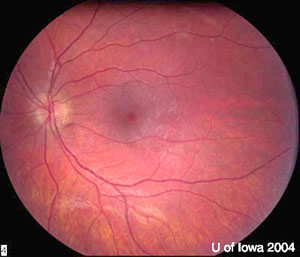
Visual acuity was 20/25 bilaterally with clear corneas and no fundus abnormalities. A diagnosis of Chronic Progressive External Ophthalmoplegia (CPEO) was made.
Disease Entity
Chronic Progressive External Ophthalmoplegia (CPEO) represents a mitochondrial myopathy primarily targeting extraocular muscles and levators.
Ophthalmologists encounter this condition due to its hallmark bilateral ptosis and ophthalmoplegia, which demand precise diagnosis to differentiate from acute or inflammatory disorders.
Early recognition prevents misdiagnosis as myasthenia gravis or thyroid eye disease. CPEO often progresses insidiously, impairing quality of life through functional visual obstruction and mobility limitations.
As a core feature of mitochondrial cytopathies, it requires multidisciplinary input but starts with ophthalmic evaluation. Clinicians must assess for systemic involvement to guide referrals.
Pathophysiology
CPEO arises from mitochondrial DNA (mtDNA) mutations, typically large-scale deletions affecting oxidative phosphorylation.
Mitochondria in muscle cells accumulate dysfunctional copies, leading to energy failure in high-demand tissues like extraocular muscles.
Step one involves sporadic or inherited mtDNA deletions, often in genes encoding tRNA or respiratory chain subunits.
This triggers impaired ATP production, causing ragged-red fibers on biopsy—clusters of subsarcolemmal mitochondria.
Extraocular muscles suffer first due to their high oxidative needs and fiber-type composition. Levator palpebrae superioris weakens symmetrically, producing ptosis.
Ophthalmoplegia follows as the superior and inferior recti degenerate, sparing the pupillary constrictors reliant on glycolysis.
Secondary effects include reactive oxygen species buildup, accelerating myopathy. In CPEO-plus, nuclear gene mutations disrupt mtDNA maintenance, broadening involvement to skeletal muscle and nerves.
Epidemiology
CPEO manifests typically in early adulthood, with onset between 20 and 40 years. Symptoms rarely appear before adolescence or after 60.
Gender distribution shows no strong predilection, though sporadic cases slightly favor females due to maternal mtDNA inheritance.
Risk factors include family history of mitochondrial disorders, as 20-30% inherit mutations maternally. Sporadic deletions account for most cases, linked to aging or oxidative stress.
Prevalence remains rare, estimated at 1:20,000 in adults, higher in mitochondrial clinic cohorts. Early onset correlates with larger deletions and worse prognosis. No ethnic bias emerges clearly.
Clinical Features
- Bilateral ptosis, often symmetric and progressive, leading to compensatory brow elevation.
- Gradual ophthalmoplegia starting with vertical gaze limitation, especially upgaze restriction.
- Insidious onset in the third or fourth decade, advancing over the years without acute exacerbations.
- Absence of diplopia in many due to symmetric involvement and head compensation.
- Mild proximal limb weakness in 50% of cases, rarely causing the initial complaint.
- Associated sensorineural hearing loss, dysphagia, or ataxia in CPEO-plus forms.
- No pain, proptosis, or pupil involvement, distinguishing from inflammatory etiologies.
Examination Findings
- Visual acuity is preserved at 20/20 to 20/40 unless comorbid retinopathy exists.
- Anterior segment normal; exposure keratopathy possible from severe ptosis and lagophthalmos.
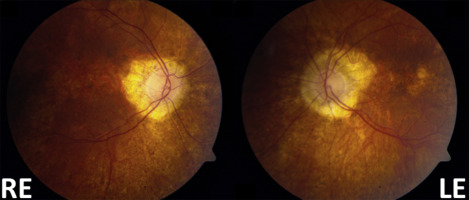
- Fundus exam shows salt-and-pepper retinopathy or optic atrophy in 10-20% of advanced cases.
- Extraocular motility severely limited: upgaze absent, downgaze reduced, horizontal variable.
- Ptosis metrics: vertical fissure height 2-4 mm, levator function <4 mm, poor Bell phenomenon.
- Orbital MRI reveals extraocular muscle atrophy, up to 43% volume loss.
- OCT demonstrates outer retinal thinning or optic nerve head volume reduction in select patients.
Differential Diagnosis
– Ocular myasthenia gravis: fatigable ptosis, diplopia, positive ice test.
– Thyroid-associated ophthalmopathy: proptosis, lid retraction, restrictive pattern.
– Congenital fibrosis of extraocular muscles (CFEOM): static deficits from birth.
– Kearns-Sayre syndrome: earlier onset with retinopathy, heart block.
– Myotonic dystrophy: cataract, orbicularis weakness, systemic features.
– Brainstem stroke or tumor: acute, asymmetric, pupil involvement.
– Progressive supranuclear palsy: vertical gaze palsy with Parkinsonism.
Diagnosis
Clinicians establish CPEO diagnosis through characteristic bilateral ptosis and painless ophthalmoplegia without pupil or pain features.
History emphasizes slow progression and family mitochondrial traits. Imaging like orbital MRI confirms extraocular muscle atrophy, supporting exclusion of mass lesions.
Muscle biopsy reveals ragged-red fibers and mtDNA deletions, the gold standard for confirmation. Serum lactate elevation aids but lacks specificity.
Genetic testing identifies mtDNA deletions in 70% of cases; negative blood tests prompt skeletal muscle analysis. Electromyography shows myopathic changes. Rule out mimics with antibody panels and thyroid function.
Management
Observation:
Monitor stable cases with serial motility and ptosis assessments every 6-12 months. Educate on head positioning and lubrication to prevent keratopathy.
Medical Treatment:
No disease-modifying therapy exists. Coenzyme Q10 supplementation may enhance mitochondrial function in deficient patients. Address keratopathy with lubricants and taping.
Refer for hearing aids or cardiac evaluation in CPEO-plus.
Surgical Treatment:
Reserve ptosis surgery for severe functional impairment after oculoplastic consultation. Frontalis sling with autogenous fascia or silicone rod corrects poor levator function, avoiding overcorrection to prevent lagophthalmos.
Strabismus surgery is rarely indicated due to the absence of diplopia. Prism glasses manage rare intermittent deviations post-orthoptic evaluation.
Prognosis
Visual acuity remains stable long-term, with threats from exposure keratopathy rather than central vision loss. Progression confines eyes to the primary position, relying on head turns.
Prognostic factors include onset age—earlier starts predict faster decline—and deletion size. CPEO-plus variants worsen with systemic features like cardiomyopathy. Life expectancy is normal, absent cardiac conduction defects.
Prevention
No primary prevention exists due to genetic etiology. Screen family members with ptosis or ophthalmoplegia via clinical exam and genetic testing.
Avoid mitochondrial toxins like alcohol excess in at-risk individuals. Prenatal counseling informs reproductive risks in maternal inheritance.
Conclusion
CPEO demands vigilant ophthalmic recognition of progressive ptosis and ophthalmoplegia amid mitochondrial dysfunction.
Prioritize biopsy-confirmed diagnosis, symptomatic ptosis correction, and keratopathy prevention. Ophthalmologists drive initial management, coordinating multidisciplinary care for optimal outcomes.
Would you have interest in taking retinal images with your smartphone?
Fundus photography is superior to fundus analysis as it enables intraocular pathologies to be photo-captured and encrypted information to be shared with colleagues and patients.
Recent technologies allow smartphone-based attachments and integrated lens adaptors to transform the smartphone into a portable fundus camera and Retinal imaging by smartphone.
RETINAL IMAGING BY YOUR SMARTPHONE
References
1. Hamilton Health Sciences. Chronic Progressive External Ophthalmoplegia (CPEO). Clinical handout.
2. EyeWiki. Chronic Progressive External Ophthalmoplegia (CPEO). American Academy of Ophthalmology.
3. MedlinePlus Genetics. Progressive External Ophthalmoplegia.
4. Yu-Wai-Man P, et al. Ophthalmoplegia. In: Ryan SJ, ed. Retina. 5th ed. Saunders; 2013.
5. Sadun AA, et al. Mitochondrial ophthalmoplegia. Surv Ophthalmol. 2011;56(3):248-267.

{kind=link}