
Case Presentation
A 72-year-old female presented with an acute onset of severe right eye pain, redness, and profound vision loss over the past 48 hours.


Her medical history included untreated cataracts for over a decade and no prior ocular surgeries or systemic comorbidities.
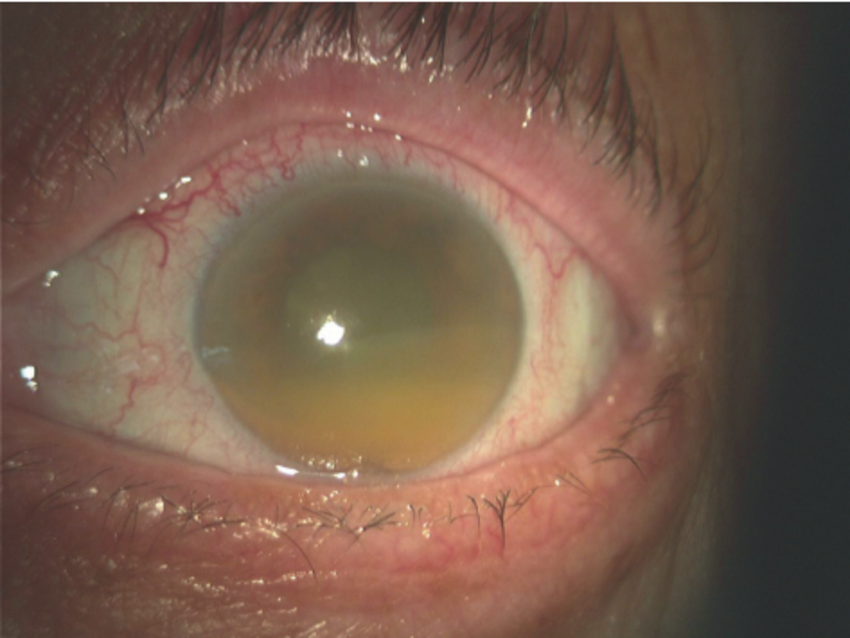
On examination, visual acuity was hand motion in the right eye and 20/30 in the left. Slit-lamp evaluation revealed a deep anterior chamber with 2+ flare, 3+ large translucent cells, and white flocculent material.
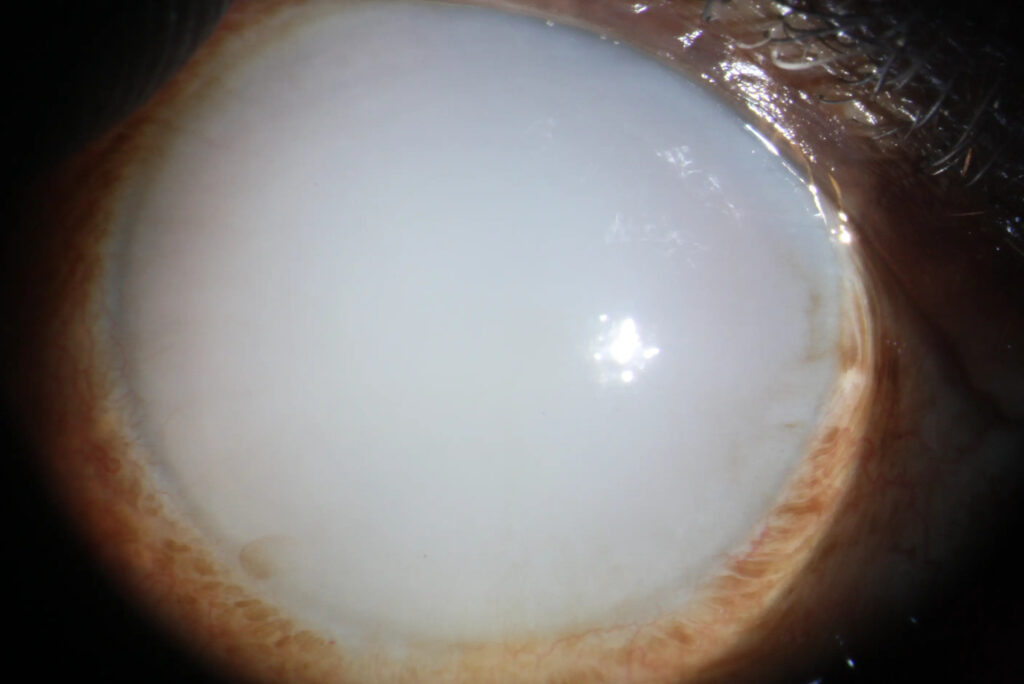
The right lens showed a hypermature cataract with a sunken sclerotic nucleus and phacodonesis.
Intraocular pressure measured 52 mmHg in the right eye via tonopen, with open angles on gonioscopy and mild corneal edema. A diagnosis of Phacolytic Glaucoma was made.
Disease Entity
Phacolytic glaucoma represents a secondary open-angle glaucoma arising from a hypermature cataract.
Ophthalmologists encounter this condition in patients with neglected cataracts, where lens protein leakage triggers acute intraocular pressure elevation.
Clinicians must recognize it promptly, as it threatens optic nerve integrity and corneal endothelium. Delayed intervention risks permanent vision loss.
This entity underscores the urgency of cataract surgery in advanced cases, distinguishing it from primary glaucomas.
Early identification prevents complications like optic neuropathy and endothelial decompensation.
Pathophysiology
Hypermature cataracts initiate the process through cortical liquefaction. Proteases A and B degrade high molecular weight lens proteins into soluble fragments. These proteins diffuse through microperforations in the intact lens capsule.
Lens proteins enter the anterior chamber, provoking an immune response. Large macrophages form, engulfing liquefied cortex material. These cells appear translucent and oversized, depositing on the lens capsule.
High molecular weight proteins accumulate directly in the trabecular meshwork. They mechanically obstruct aqueous outflow, independent of macrophages. This blockage elevates intraocular pressure acutely.
Inflammatory cells contribute minimally. Fibrinogen presence promotes adhesions, though synechiae remain rare. The lens nucleus sinks inferiorly, creating a morgagnian cataract configuration.
Vascular endothelial damage follows prolonged pressure spikes. Optic nerve head excavation progresses rapidly. Corneal edema develops from endothelial cell loss.
Epidemiology
Phacolytic glaucoma predominantly affects elderly patients over 60 years. Typical age group spans 65 to 80 years, reflecting cataract maturation time.
Gender distribution shows no strong predilection. Both males and females present equally, linked to cataract neglect rather than sex-specific factors.
Risk factors center on untreated hypermature cataracts. Long-standing cataracts in developing regions heighten incidence due to surgical access barriers.
Ocular trauma history confounds diagnosis occasionally. Comorbidities like diabetes accelerate cataract progression. Delayed healthcare seeking amplifies risk.
Clinical Features
- Acute onset of severe ocular pain, often unilateral.
- Redness and photophobia accompany inflammation.
- Profound vision loss, from counting fingers to light perception.
- Symptoms progress rapidly over hours to days.
- Gradual vision decline precedes an acute episode in chronic cataracts.
- Unilateral involvement predominates; bilateral rare unless symmetric cataracts.
- Halos around lights occur from corneal edema.
- No systemic symptoms typically.
Examination Findings
- Visual acuity is severely reduced, often to hand motion or worse.
- The anterior segment shows a deep chamber with flare and large cells.
- White flocculent material floats in aqueous humor.
- Hypermature cataract with phacodonesis or morgagnian nucleus.
- Mild to moderate corneal edema is present.
- Gonioscopy reveals open angles, no synechiae.
- Fundus view obscured; optic disc cupping if chronic.
- OCT demonstrates peripapillary nerve fiber layer thinning in advanced cases.
- Fluorescein angiography is rarely indicated; B-scan shows no posterior pathology.
Differential Diagnosis
- Phacomorphic glaucoma: shallow anterior chamber, angle closure.
- Angle recession glaucoma: trauma history, recessed angle.
- Lens particle glaucoma: disrupted capsule, lens fragments.
- Phacoantigenic glaucoma: intense uveitis, keratic precipitates.
- Primary open-angle glaucoma: no cataract, insidious onset.
- Neovascular glaucoma: iris neovascularization, diabetes history.
- Uveitic glaucoma: posterior synechiae, small cells.
Diagnosis
Clinicians diagnose phacolytic glaucoma clinically. Key features include hypermature cataract, open angles, elevated intraocular pressure, and anterior chamber inflammation with large macrophages.
Imaging supports confirmation. Slit-lamp biomicroscopy identifies lens morphology and cells. Gonioscopy excludes angle closure. B-scan ultrasonography rules out posterior segment pathology.
Ancillary tests prove adjunctive. Tonometry quantifies pressure spikes. Endothelial cell count assesses corneal risk. Aqueous tap is rarely needed but reveals lens proteins.
Management
Observation
Observation suits minimal pressure elevation without symptoms. Monitor closely in early hypermature stages. Avoid if IOP exceeds 30 mmHg or vision threatens.
Medical Treatment
Initiate aggressive IOP reduction promptly. Topical beta-blockers lower aqueous production. Alpha-2 agonists and carbonic anhydrase inhibitors provide an additive effect. Oral acetazolamide achieves rapid control.
Topical steroids mitigate inflammation. Prednisolone acetate 1% every 2 hours reduces cell and flare. Cycloplegics prevent synechiae formation.
Surgical Treatment
Cataract extraction offers a definitive cure. Extracapsular cataract extraction removes a hypermature lens. Posterior chamber intraocular lens implantation follows.
Perform urgently after IOP stabilization. Endothelial protection is crucial via viscoelastics. Pars plana vitrectomy if vitreous involvement is suspected.
Postoperative IOP agents continue if needed. An anti-inflammatory regimen prevents rebound.
Prognosis
Visual outcome improves markedly post-surgery. Most regain 20/40 or better if the optic nerve spares. Persistent cupping limits recovery in delayed cases.
Prognostic factors include presentation IOP, duration, and preoperative disc damage. Corneal decompensation worsens the outlook. Early intervention yields the best results.
Follow-up monitors IOP weekly initially, then monthly. Assess endothelial density and optic coherence tomography for progression.
Prevention
Control risk through timely cataract surgery. Screen elderly patients annually in high-risk populations. Educate on cataract progression dangers.
Promote surgical access in underserved areas. Manage comorbidities like diabetes to slow cataract maturation.
HOW TO TAKE SLIT-LAMP EXAM IMAGES WITH A SMARTPHONE?
Smartphone slit-lamp photography is the new advancement in the field of science and technology in which photographs of the desired slit-lamp finding can be taken with smartphones by using the slit-lamp adapters.
Slit-lamp Smartphone photography
References
1. Chandler PA, Grant RP. Phacolytic glaucoma. Am J Ophthalmol. 1955;40(3):167-171.
2. Epstein DL, Jedziniak G, Grant RP. Obstruction of aqueous outflow by high molecular weight lens proteins. Invest Ophthalmol Vis Sci. 1978;17(2):93-97.
3. Flocks M, Litt GJ, Zimmerman LE. Phacolytic glaucoma: a clinicopathologic study of fifty-eight cases. Arch Ophthalmol. 1955;54(1):37-45.
4. EyeRounds.org. Phacolytic Glaucoma Case. University of Iowa; 2020.
5. Rhee DJ. Diagnosis and Management of Phacolytic Glaucoma. Glaucoma Today. 2018;16(4):32-35.

{kind=link}