
Case study
A 52-year-old woman presented with a 6-month history of progressively worsening bilateral ocular dryness, foreign body sensation, and intermittent blurred vision, particularly in low-humidity environments.

She reported associated dry mouth, difficulty swallowing dry foods, and mild joint pains but denied recent infections or new medications.
Her medical history included mild hypothyroidism managed with levothyroxine and no prior ocular surgery. On examination, visual acuity was measured at 20/40 bilaterally.
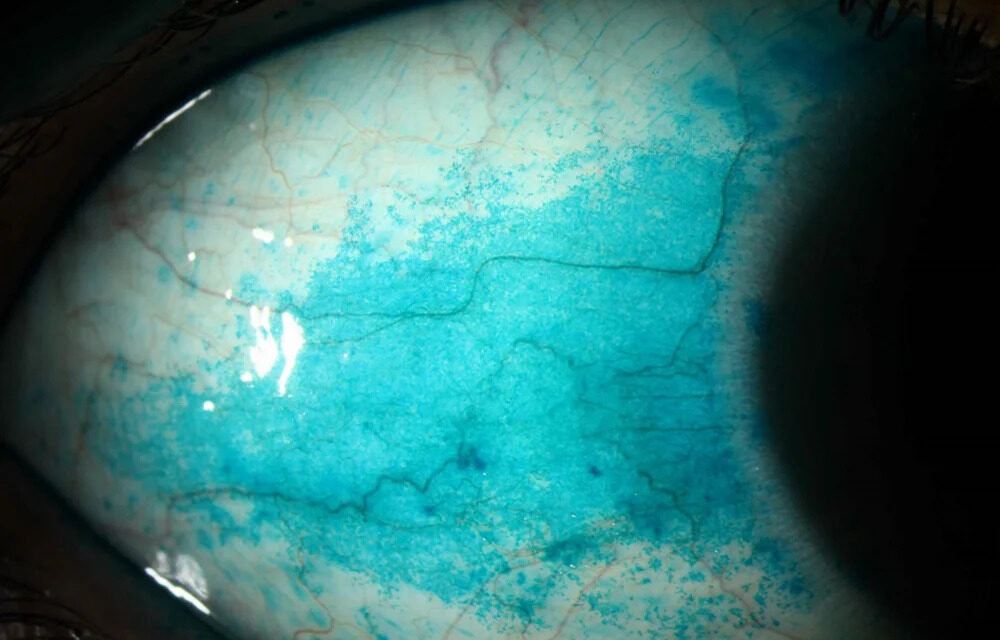
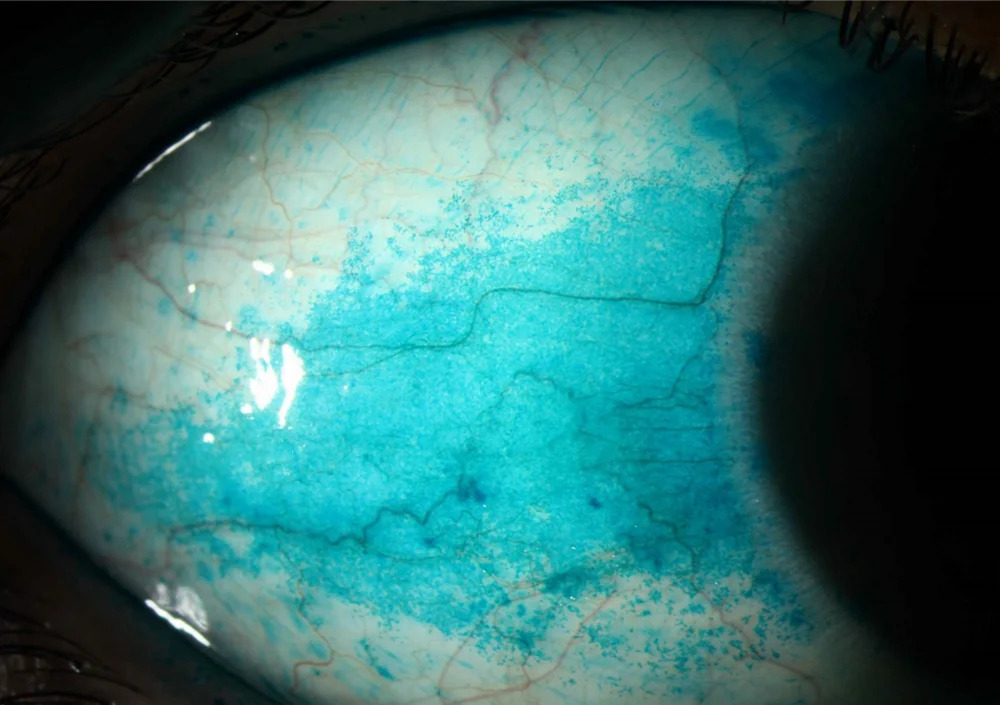
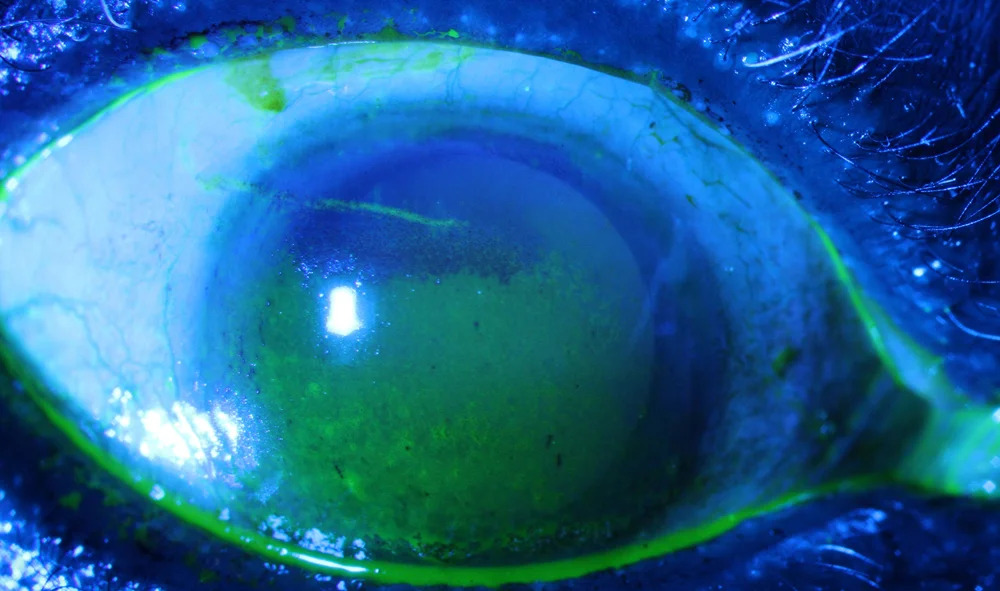
Schirmer test showed 2 mm wetting in 5 minutes OU, slit-lamp revealed punctate epithelial erosions and filamentary keratitis on the corneal surface with mild conjunctival injection, and tear breakup time was less than 5 seconds.
A diagnosis of Sjögren’s Syndrome was made.
Disease Entity
Sjögren’s Syndrome (SS) represents a chronic autoimmune disorder primarily targeting exocrine glands, leading to diminished tear and saliva production.
Ophthalmologists encounter SS most frequently through its hallmark ocular manifestation: severe aqueous-deficient dry eye disease, or keratoconjunctivitis sicca (KCS).
This condition demands attention because KCS in SS often proves refractory to standard dry eye therapies, risking corneal complications like ulceration or perforation.
Early recognition by ophthalmologists enables multidisciplinary care, averting vision-threatening sequelae and systemic complications such as lymphoma.
SS affects ocular surface homeostasis profoundly, distinguishing it from other dry eye etiologies through its autoimmune-driven glandular destruction.
Pathophysiology
Autoimmune lymphocytic infiltration targets lacrimal acinar cells first, initiating glandular atrophy. T and B lymphocytes form periductal foci, disrupting tear secretion via cytokine release, including IL-1, IL-6, TNF-α, and IFN-γ. This aqueous deficiency destabilizes the tear film, exposing the ocular surface to hyperosmolarity and inflammation.
Conjunctival goblet cells decrease, impairing mucin production and exacerbating epithelial damage. Meibomian glands suffer secondary inflammation, altering lipid layer stability and promoting evaporative loss.
Corneal nerves undergo neuropathy, reducing sensation and perpetuating a cycle of poor blinking and exposure.
In advanced stages, filamentary keratitis arises from mucus adhesion to devitalized epithelium.
Vascular changes remain minimal, but chronic inflammation may induce subclinical scleritis or uveitis in severe cases.
Epidemiology
SS predominantly affects middle-aged to older adults, with peak onset between 40 and 60 years. Women comprise 90% of cases, yielding a 9:1 female-to-male ratio.
Risk factors include genetic predisposition via HLA-DR3 and HLA-DQw2 alleles, environmental triggers like viral infections (Epstein-Barr virus), and hormonal influences post-menopause.
Secondary SS associates with rheumatoid arthritis or systemic lupus erythematosus in 20-30% of patients.
Prevalence estimates reach 0.5-1% in the general population, with underdiagnosis common due to insidious onset.
Clinical Features
Symptoms center on bilateral ocular dryness, manifesting as grittiness, burning, itching, and foreign body sensation.
Photophobia and eye fatigue worsen in dry or windy conditions; blurred vision fluctuates with blinking.
Onset proves insidious, progressing over months to years; acute exacerbations occur with anticholinergic drugs or low humidity.
Bilateral involvement predominates, though asymmetry arises early. Associated sicca symptoms include xerostomia; systemic features like arthralgia or parotid swelling prompt ophthalmologic consultation.
Progression leads to corneal pain and reduced quality of life, disproportionate to visible signs.

Examination Findings
- Visual acuity often reduces to 20/40 or worse bilaterally due to tear film instability.
- Anterior segment shows conjunctival hyperemia, superior limbic keratoconjunctivitis, and chalasis.
- Corneal punctate erosions predominate inferiorly; filamentary keratitis appears in moderate cases.
- Fundus examination remains normal unless rare vasculitis or optic neuritis complicates.
- Schirmer test yields less than 5 mm/5 min OU, confirming aqueous deficiency.
- Tear breakup time measures under 10 seconds; vital staining (fluorescein, rose bengal) reveals epithelial defects.
- OCT demonstrates attenuated tear meniscus height and irregular epithelium; confocal microscopy shows subbasal nerve loss.
Differential Diagnosis
- Age-related aqueous-deficient dry eye.
- Blepharitis-associated evaporative dry eye.
- Drug-induced sicca (anticholinergics, antihistamines).
- Graft-versus-host disease post-transplant.
- Chronic Stevens-Johnson syndrome sequelae.
- Ocular rosacea with meibomian dysfunction.
- Primary ciliary dyskinesia or congenital alacrima.
- Neurologic causes, like trigeminal neuropathy.
Diagnosis
Clinical diagnosis hinges on sicca symptoms plus objective ocular evidence of KCS. Schirmer test less than 5 mm/5 min and positive vital staining (rose bengal or lissamine green score ≥4) establishes ocular involvement.
Ancillary tests include anti-SSA/Ro and anti-SSB/La antibodies, which are elevated in 70% of primary SS.
Labial salivary gland biopsy confirms lymphocytic foci (focus score ≥1/4 mm²). Imaging, like salivary ultrasonography, detects glandular inhomogeneity but plays an adjunctive role.
Ophthalmologists contribute via Ocular Surface Disease Index scoring and tear osmolarity (>308 mOsm/L). ACR/EULAR criteria integrate these for classification, emphasizing biopsy and serology.
Management
Observation:
Monitor mild cases quarterly with Schirmer and staining assessments. Advise environmental modifications: humidifiers, wraparound sunglasses, and omega-3 supplementation.
Medical Treatment:
Initiate preservative-free artificial tears every 2 hours. Escalate to cyclosporine 0.05-0.09% emulsion twice daily to suppress inflammation.
Lifitegrast 5% inhibits T-cell activation. Autologous serum tears (20-50%) deliver growth factors for severe KCS. Punctal occlusion with plugs or cautery preserves tears.
Oral pilocarpine or cevimeline stimulates secretion in glandular function remnants. Systemic immunosuppressants (hydroxychloroquine, methotrexate) address the autoimmune drive; rituximab targets B-cells in refractory cases.
Surgical Treatment:
Lateral tarsorrhaphy protects severe filamentary keratitis. Amniotic membrane transplantation aids epithelial healing. PROSE scleral lenses vault the cornea, stabilizing tears. Keratoprosthesis serves end-stage perforation.
Prognosis
Visual outcomes remain favorable with early intervention, preserving 20/25 acuity in 80% of compliant patients.
Prognostic factors include disease duration, baseline Schirmer value, and autoantibody status; anti-SSA positivity predicts severity.
Corneal scarring or vascularization threatens 10-20% without treatment. Regular follow-up every 3-6 months tracks progression and lymphoma risk (5% lifetime). Multidisciplinary surveillance optimizes outcomes.
Prevention
No primary prevention exists due to autoimmune etiology. Screen high-risk patients (sicca plus arthralgia) with Schirmer and serology during routine exams.
Control modifiable risks: avoid smoking, limit anticholinergics. Early hydroxychloroquine in positive autoantibodies may halt glandular destruction.
HOW TO TAKE SLIT-LAMP EXAM IMAGES WITH A SMARTPHONE?
Smartphone slit-lamp photography is the new advancement in the field of science and technology in which photographs of the desired slit-lamp finding can be taken with smartphones by using the slit-lamp adapters.
Slit-lamp Smartphone photography
References
1. Fox RI. Clinical manifestations and early diagnosis of Sjögren syndrome. Arch Intern Med. 2005;165(12):1275-1283.
2. Vivino FB, et al. Sjögren’s syndrome: an update on disease pathogenesis, clinical management and future directions. Front Immunol. 2021;12:799785.
3. Shiboski CH, et al. 2016 American College of Rheumatology/European League Against Rheumatism classification criteria for primary Sjögren’s syndrome. Arthritis Rheumatol. 2017;69(1):35-45.
4. Akpek EK, et al. Dry eye in Sjögren’s syndrome. EyeWiki. American Academy of Ophthalmology. Accessed 2023.
5. Sall K, et al. Cyclosporine emulsion 0.05% for severe dry eye associated with Sjögren’s syndrome. Ophthalmology. 2000;107(5):915-921.

{kind=link}