
Case Study
A 58-year-old male presented to the retina clinic with a 2-week history of progressive, painless visual loss in his left eye.


He described a dark shadow spreading from the inferior visual field upward, associated with mild metamorphopsia. There was no history of ocular trauma or prior retinal surgery.
His medical history was notable for poorly controlled hypertension and a recent diagnosis of choroidal melanoma in the same eye, for which he was under systemic evaluation.
Examination Results:
-
Visual Acuity: 20/25 in the right eye and counting fingers at 2 meters in the left eye
-
Anterior Segment: Unremarkable in both eyes
-
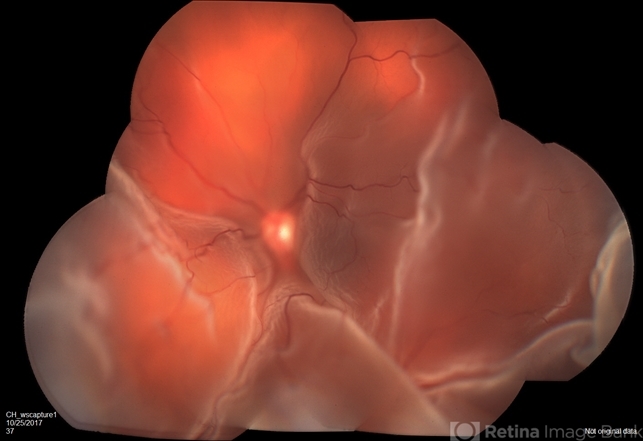
Fundus Examination: Smooth, dome-shaped elevation of the neurosensory retina involving the posterior pole without retinal breaks
-
Optical Coherence Tomography (OCT): Extensive subretinal fluid with an intact but elevated neurosensory retina
-
B-scan Ultrasonography: Choroidal thickening with associated exudative retinal detachment
-
Fluorescein Angiography: Late pooling of dye without evidence of retinal tears
A diagnosis of Bullous Retinal Detachment secondary to choroidal pathology was established.
Disease Entity
Bullous retinal detachment refers to a form of retinal detachment characterized by a smooth, convex, and often rapidly progressive elevation of the neurosensory retina due to the accumulation of subretinal fluid.
Unlike rhegmatogenous retinal detachment, bullous retinal detachment typically occurs without retinal breaks and is most commonly associated with exudative or tractional mechanisms.
The detachment often appears highly elevated, mobile, and dome-shaped, giving it the characteristic “bullous” configuration.
This type of detachment is frequently linked to inflammatory, vascular, neoplastic, or systemic conditions that disrupt the balance of fluid movement across the retinal pigment epithelium (RPE).
Pathophysiology
The pathophysiology of bullous retinal detachment centers on excessive accumulation of subretinal fluid due to impaired resorption or increased leakage.
Key mechanisms include:
-
Breakdown of the outer blood-retinal barrier at the level of the RPE
-
Increased choroidal vascular permeability
-
Inflammatory or neoplastic infiltration of the choroid
-
Reduced RPE pump function
In exudative bullous detachments, fluid originates primarily from the choroidal circulation rather than the vitreous cavity.
Conditions such as uveal tumors, inflammatory choroiditis, or systemic vascular disorders increase hydrostatic pressure or permeability, allowing fluid to accumulate beneath the retina.
Because no retinal break is present, the detachment often shifts with changes in head position.
Epidemiology
Bullous retinal detachment is not a distinct disease but rather a clinical manifestation seen in various ocular and systemic disorders.
It may occur at any age, depending on the underlying cause. Inflammatory causes are more common in younger patients, while neoplastic and vascular etiologies predominate in older adults.
The true incidence is difficult to quantify due to its heterogeneous causes and frequent misclassification as rhegmatogenous retinal detachment in early stages.

Etiology
Common causes of bullous retinal detachment include:
-
Choroidal tumors: Choroidal melanoma, hemangioma, metastasis
-
Inflammatory diseases: Vogt–Koyanagi–Harada disease, posterior scleritis
-
Vascular disorders: Severe hypertensive choroidopathy, preeclampsia
-
Infectious conditions: Posterior uveitis, choroiditis
-
Idiopathic causes: Central serous chorioretinopathy variants
Recognition of the underlying etiology is essential for appropriate management.
Clinical Features
Patients with bullous retinal detachment commonly present with:
-
Rapid or subacute vision loss
-
Visual field defects described as shadows or curtains
-
Metamorphopsia
-
Reduced contrast sensitivity
Pain is usually absent unless associated with inflammatory causes such as posterior scleritis.
On examination, the retina appears smooth, elevated, and mobile, often shifting with eye or head movement.
Examination Findings
Fundus Examination:
-
Smooth, convex retinal elevation
-
Absence of retinal tears or holes
-
Possible underlying choroidal mass or inflammation
Optical Coherence Tomography (OCT):
-
Large amounts of subretinal fluid
-
Intact neurosensory retina
-
Possible RPE irregularities
Fluorescein Angiography:
-
Late pooling of dye
-
Absence of leakage from retinal breaks
B-scan Ultrasonography:
-
Essential for detecting choroidal pathology
-
Helps differentiate exudative from tractional causes
Differential Diagnosis
Bullous retinal detachment must be differentiated from:
-
Rhegmatogenous retinal detachment
-
Tractional retinal detachment
-
Central serous chorioretinopathy
-
Choroidal effusion
-
Suprachoroidal hemorrhage
Careful imaging and examination are critical to avoid unnecessary surgical intervention.
Diagnosis
Diagnosis is based on:
-
Detailed fundus examination
-
Multimodal imaging, including OCT, FFA, and B-scan ultrasound
-
Systemic evaluation when indicated
Identifying the absence of retinal breaks is a key diagnostic feature.
Management
Management of bullous retinal detachment focuses on treating the underlying cause rather than immediate retinal surgery.
Treatment options include:
-
Corticosteroids: Systemic or local for inflammatory causes
-
Anti-VEGF therapy: In selected vascular conditions
-
Tumor-directed therapy: Radiotherapy or systemic oncology management
-
Systemic control: Blood pressure management, treatment of systemic disease
Surgical retinal reattachment is generally not indicated unless secondary rhegmatogenous detachment develops.
Prognosis
Visual prognosis depends largely on:
-
Duration of detachment
-
Involvement of the macula
-
Underlying etiology
Early recognition and treatment of the primary cause can lead to significant visual recovery. Chronic bullous detachments may result in permanent photoreceptor damage and visual loss.
Prevention
Prevention focuses on:
-
Early detection of systemic and ocular diseases
-
Prompt referral to retina specialists
-
Regular follow-up for high-risk patients
Effective systemic disease control plays a crucial role in reducing recurrence.
Conclusion
Bullous retinal detachment is a distinctive clinical presentation that reflects underlying choroidal or systemic pathology rather than a primary retinal break.
Accurate diagnosis, careful differentiation from other types of retinal detachment, and targeted management of the underlying cause are essential to preserve vision and avoid unnecessary surgical intervention.
Would you have interest in taking retinal images with your smartphone?
Fundus photography is superior to fundus analysis as it enables intraocular pathologies to be photo-captured and encrypted information to be shared with colleagues and patients.
Recent technologies allow smartphone-based attachments and integrated lens adaptors to transform the smartphone into a portable fundus camera and Retinal imaging by smartphone.
RETINAL IMAGING BY YOUR SMARTPHONE
References
-
Ryan SJ, Schachat AP, Wilkinson CP. Retina. Elsevier.
-
Shields CL, Shields JA. Choroidal tumors and exudative retinal detachment. Survey of Ophthalmology.
-
Gass JD. Differential diagnosis of retinal detachment. American Journal of Ophthalmology.
-
Spaide RF. Diseases of the choroid and exudative retinal detachment. Retina.

{kind=link}