
Case Study
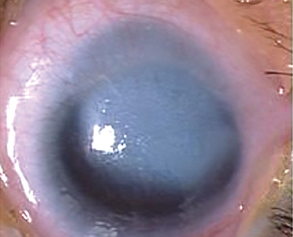
A 4-month-old infant was referred for evaluation of bilateral cloudy corneas since birth. The parents reported no history of infection or trauma during pregnancy.


On examination, both corneas showed central opacification with a clear peripheral cornea. The anterior chambers were shallow, and iridocorneal adhesions were visible.
Lens opacity was present in one eye. Intraocular pressure was normal, but corneal diameter was slightly reduced.
Ultrasound biomicroscopy revealed the absence of Descemet’s membrane and posterior corneal stroma in the central area.
Based on these findings, the diagnosis of Peters Anomaly was established, a rare congenital defect characterized by abnormal anterior segment development.
Disease Entity
Peters Anomaly is a rare congenital disorder involving defective development of the anterior segment of the eye, primarily affecting the cornea, iris, and lens.
It is a form of anterior segment dysgenesis (ASD) that manifests as central corneal opacity and abnormalities in the posterior corneal stroma, Descemet’s membrane, and endothelium.
Depending on the severity, adhesions between the iris and cornea and even the lens and cornea may occur.
Pathophysiology
Peters Anomaly arises from abnormal migration and differentiation of neural crest cells during the fifth to sixth week of gestation.
.These cells are responsible for forming the corneal endothelium, stroma, and anterior chamber angle structures.
Incomplete separation of the lens vesicle from the surface ectoderm disrupts anterior segment formation, resulting in maldevelopment of the posterior cornea and adjacent structures.
Two main subtypes are recognized:
-
Type I Peters Anomaly: Corneal opacity with iridocorneal adhesions, but the lens is clear and separated from the cornea.
-
Type II Peters Anomaly: Corneal opacity with lens abnormalities, including lenticulocorneal adhesions or cataract.
Genetic mutations in several genes, such as PAX6, PITX2, FOXC1, CYP1B1, and B3GALTL, have been implicated in the disease, and Peters Anomaly can occur as part of systemic syndromes like Axenfeld-Rieger syndrome or Peters Plus syndrome.
Epidemiology
Peters Anomaly is rare, with an estimated incidence of 1 in 100,000 live births. It can occur sporadically or follow autosomal recessive or dominant inheritance patterns depending on the gene involved.
Approximately 60–70% of cases are bilateral, and up to 50% have associated ocular or systemic abnormalities.
Clinical Features
The hallmark of Peters Anomaly is central corneal opacity present at birth. The degree of opacification varies, affecting visual potential.
Ocular manifestations include:
-
Central or paracentral corneal opacity with clear peripheral cornea.
-
Absence of Descemet’s membrane and posterior stroma in the affected area.
-
Iris strands adherent to the posterior cornea (iridocorneal adhesions).
-
Lens abnormalities, including cataract or lenticulocorneal adhesion.
-
Shallow anterior chamber and microcornea.
-
Secondary glaucoma occurs in up to 50% of cases.
Systemic associations may include:
-
Craniofacial anomalies.
-
Cleft lip or palate.
-
Cardiac, genitourinary, and skeletal malformations (notably in Peters Plus syndrome).
Examination Findings
Anterior Segment:
-
Central corneal leukoma with varying density.
-
Iridocorneal or lenticulocorneal adhesions are visible under slit-lamp or gonioscopy.
-
Shallow anterior chamber in severe cases.
Posterior Segment:
-
Fundus may appear normal if corneal clarity allows visualization.
-
Ultrasound B-scan or OCT may show normal posterior pole anatomy when media opacity obscures the view.
Imaging:
-
Ultrasound Biomicroscopy (UBM): Reveals defects in the posterior cornea and adhesion patterns.
-
Anterior Segment OCT: Confirms absence of Descemet’s membrane and stromal thinning.
Other Findings:
-
Elevated intraocular pressure in secondary glaucoma.
-
Abnormal corneal diameter (microcornea).
Differential Diagnosis
Conditions that can mimic Peters Anomaly include:
-
Congenital hereditary endothelial dystrophy (CHED): Diffuse corneal opacity without adhesions.
-
Sclerocornea: Peripheral corneal opacification with vascularization.
-
Congenital glaucoma: Corneal edema with enlarged corneal diameter.
-
Anterior segment dysgenesis syndromes, Such as Axenfeld-Rieger syndrome.

Diagnosis
The diagnosis of Peters Anomaly is based on a combination of clinical findings and imaging studies.
Key diagnostic criteria include:
-
Central corneal opacity present at birth.
-
Absence or thinning of Descemet’s membrane and posterior stroma.
-
Iridocorneal or lenticulocorneal adhesions are visible clinically or on imaging.
-
Genetic testing confirming mutations in PAX6, PITX2, FOXC1, or B3GALTL.
Systemic evaluation is recommended to rule out associated syndromic anomalies.
Management
The management of Peters Anomaly aims to restore visual function, manage complications, and prevent amblyopia.
1. Medical Management:
-
Treatment of glaucoma: Topical or surgical management (trabeculotomy, goniotomy).
-
Lubricants and anti-inflammatory drops: To maintain corneal comfort and prevent scarring.
-
Amblyopia therapy: Early visual rehabilitation is critical in unilateral cases.
2. Surgical Management:
-
Penetrating Keratoplasty (PK): The mainstay treatment for visual rehabilitation in dense corneal opacities. The success rate is lower in infants due to graft rejection, postoperative infection, and glaucoma.
-
Keratolimbal allograft (KLAL): Used in cases with limbal stem cell deficiency.
-
Keratoprosthesis (Boston KPro): Considered in cases where multiple grafts have failed.
-
Management of adhesions: Iridocorneal or lenticulocorneal adhesions may require synechiolysis.
3. Genetic and Systemic Evaluation:
Genetic counseling is advised for affected families, particularly when systemic anomalies are present.
Prognosis
The visual prognosis varies depending on the severity of corneal opacity, presence of lens involvement, and occurrence of secondary glaucoma.
Early surgical intervention can improve visual outcomes, but postoperative complications are frequent. Lifelong follow-up is necessary for monitoring graft integrity, intraocular pressure, and amblyopia management.
Prevention
Peters Anomaly cannot be prevented, but genetic counseling and prenatal genetic testing in at-risk families may identify carriers.
Early diagnosis and prompt management can minimize the risk of irreversible visual impairment.
HOW TO TAKE SLIT-LAMP EXAM IMAGES WITH A SMARTPHONE?
Smartphone slit-lamp photography is the new advancement in the field of science and technology in which photographs of the desired slit-lamp finding can be taken with smartphones by using the slit-lamp adapters.
Slit-lamp Smartphone photography
References
-
Yang LL, Lambert SR, Drews-Botsch C, et al. Long-term visual outcome of Peters Anomaly. Ophthalmology. 2004;111(12):2270–2275.
-
Idrees F, Vaideanu D, Fraser SG, Sowden JC, Khaw PT. A review of anterior segment dysgeneses. Surv Ophthalmol. 2006;51(3):213–231.
-
Khan AO, Aldahmesh MA, Alkuraya FS. Genetic and clinical characterization of Peters anomaly in Saudi Arabia. Mol Vis. 2011;17:3190–3195.
-
Nischal KK. Management of congenital corneal opacities. Eye (Lond). 2012;26(10):1268–1276.
-
Bhandari R, Ferrone PJ, Khandelwal P, et al. Peters Anomaly: Diagnosis and management. Clin Ophthalmol. 2015;9:2127–2135.

{kind=link}