
Case Study
A 58-year-old man with a history of nasopharyngeal carcinoma presented with sudden, painless vision loss in his right eye, occurring six months after completing radiotherapy.

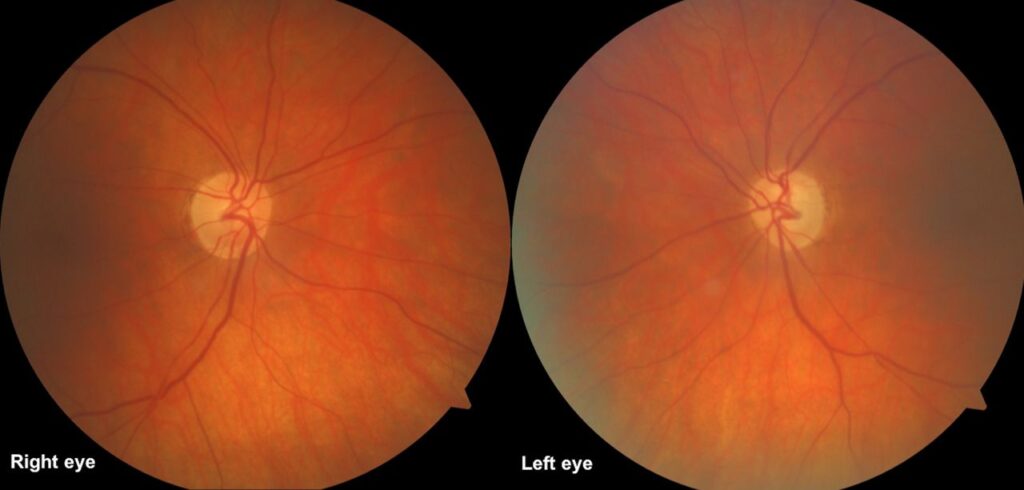
Visual acuity had dropped from 6/6 to counting fingers within a few days. Fundus examination revealed optic disc pallor with blurred margins.
Optical coherence tomography (OCT) demonstrated thinning of the retinal nerve fiber layer, and MRI excluded tumor recurrence.
Based on clinical history and findings, a diagnosis of Radiation-Induced Optic Neuropathy (RION) was made.
Disease Entity
Radiation-Induced Optic Neuropathy (RION) is a rare but devastating delayed complication of radiotherapy involving structures near the optic nerve, chiasm, or orbit.
It is characterized by sudden, painless, and often irreversible vision loss, typically occurring months to years after radiation exposure.
The condition results from vascular and axonal damage within the optic nerve due to radiation-induced ischemia and necrosis.
Pathophysiology
RION develops when high-dose ionizing radiation injures the small vessels supplying the optic nerve. This leads to occlusive vasculopathy, ischemia, demyelination, and axonal loss.
Histopathological findings reveal hyalinized vessels, demyelination, and gliosis. The risk increases when the cumulative radiation dose exceeds 50 Gy to the optic apparatus.
Concomitant chemotherapy, diabetes, and hypertension may exacerbate the damage. Unlike compressive or infiltrative optic neuropathies, RION is primarily ischemic in origin.
The latency period can vary from a few months to several years, reflecting the slow progression of vascular compromise and delayed cellular death within the optic nerve tissue.
Epidemiology
The incidence of RION is estimated to be between 0.5% and 3% in patients receiving cranial or orbital irradiation.
It typically occurs 6 to 36 months after therapy, with no gender predilection. Tumors most commonly associated include nasopharyngeal carcinoma, pituitary adenoma, meningioma, and sinonasal malignancies. Advanced radiotherapy techniques such as stereotactic radiosurgery, proton beam therapy, and intensity-modulated radiotherapy (IMRT) have reduced but not eliminated the risk.
Clinical Features
Patients usually report sudden, painless vision loss, often unilateral but occasionally bilateral when both optic nerves are within the radiation field. Visual field defects, such as central or cecocentral scotomas, are common. Some patients may retain partial peripheral vision.
On examination, the optic disc may initially appear normal but later becomes swollen and pale. With time, optic atrophy develops. Pain, inflammation, or systemic symptoms are typically absent, differentiating RION from optic neuritis or tumor recurrence.
Examination Findings (Summary):
-
Visual acuity: Severe decrease, often to counting fingers or worse
-
Pupils: Relative afferent pupillary defect (RAPD) in unilateral cases
-
Fundus: Optic disc edema progressing to pallor
-
Visual field: Central or altitudinal scotoma
-
OCT: RNFL thinning
-
MRI: Optic nerve enhancement without mass effect
Differential Diagnosis
RION can resemble several other causes of optic neuropathy. Key differentials include:
-
Optic neuritis (inflammatory demyelination)
-
Compressive optic neuropathy (tumor recurrence or metastasis)
-
Ischemic optic neuropathy (non-arteritic or arteritic)
-
Infectious optic neuropathy (toxoplasmosis, tuberculosis)
-
Infiltrative or toxic optic neuropathies

Diagnostic Approach
Diagnosis relies on clinical history of prior radiation exposure and exclusion of other causes. MRI with contrast is crucial—it typically shows enhancement and swelling of the affected optic nerve without evidence of tumor recurrence. OCT helps monitor structural changes and exclude other retinal pathologies.
Visual evoked potentials (VEP) may demonstrate reduced amplitude and delayed latency, consistent with axonal loss. Fluorescein angiography may show disc leakage in early stages.
Management
Unfortunately, there is no proven effective therapy for RION. Treatment focuses on early recognition and supportive care.
Management Strategies:
-
High-dose corticosteroids: Often used empirically in acute phases, though benefits are inconsistent.
-
Hyperbaric oxygen therapy (HBOT): May improve oxygenation and delay progression if started early.
-
Bevacizumab (anti-VEGF): Used experimentally in some cases to reduce vascular permeability.
-
Neuroprotective agents: Limited evidence, but some clinicians use antioxidants or vitamins.
-
Visual rehabilitation: Essential for patients with permanent vision loss.
Preventive measures remain the most effective strategy—limiting radiation dose to the optic nerve and chiasm, careful treatment planning, and avoiding overlapping radiation fields.

Prognosis
The prognosis of RION is generally poor, with most patients experiencing irreversible vision loss. Rarely, partial recovery occurs if intervention begins very early. Bilateral involvement predicts worse outcomes. Long-term follow-up and counseling are vital for patient adaptation to visual disability.
Prevention
Prevention is crucial, as established damage cannot be reversed. Radiation oncologists must ensure that the radiation dose to the optic apparatus stays below 50 Gy, using advanced radiotherapy planning systems to spare visual structures. Monitoring patients for early visual changes and prompt referral to ophthalmology can mitigate severe outcomes.
Would you have interest in taking retinal images with your smartphone?
Fundus photography is superior to fundus analysis as it enables intraocular pathologies to be photo-captured and encrypted information to be shared with colleagues and patients.
Recent technologies allow smartphone-based attachments and integrated lens adaptors to transform the smartphone into a portable fundus camera and Retinal imaging by smartphone.
RETINAL IMAGING BY YOUR SMARTPHONE
References
-
Miller NR, et al. Radiation-Induced Optic Neuropathy: Clinical and Pathophysiologic Review. J Neuroophthalmol.
-
Guy J, et al. Radiation Optic Neuropathy: A Review of Pathogenesis and Management. Surv Ophthalmol.
-
Danesh-Meyer HV. Radiation-Induced Optic Neuropathy: Current Understanding. Eye (Lond).
-
Parsons JT, et al. Dose-Response Relationships for Radiation-Induced Optic Neuropathy. Int J Radiat Oncol Biol Phys.
-
Levin LA. Ischemic and Radiation-Induced Optic Neuropathies: Mechanisms and Therapy. Prog Retin Eye Res.
-
Mishra KK, et al. Risk Factors and Clinical Course of Radiation Optic Neuropathy. Pract Radiat Oncol.
- RETINAL IMAGING BY YOUR SMARTPHONE

{kind=link}