
Case Study
A 34-year-old male agricultural worker from a rural area in Southeast Asia presented with severe pain, redness, and vision loss in his left eye for one week.


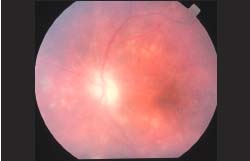
He reported a recent history of ocular trauma with a tree branch while working in the fields. Examination revealed marked conjunctival injection, corneal edema, hypopyon, and vitritis, obscuring the posterior segment view.
B-scan ultrasonography demonstrated dense vitreous opacities with membrane formation. A vitreous tap and diagnostic PCR confirmed the presence of Toxocara canis DNA.
Despite aggressive treatment with systemic albendazole, corticosteroids, and pars plana vitrectomy, the patient’s vision deteriorated to no light perception, necessitating enucleation.
Histopathology confirmed parasitic granulomatous inflammation consistent with parasitic endophthalmitis.
Disease Entity
Parasitic endophthalmitis is an uncommon but vision-threatening intraocular infection caused by the infestation of parasites within the eye.
Unlike bacterial or fungal endophthalmitis, which typically follow intraocular surgery or penetrating trauma, parasitic endophthalmitis often arises from hematogenous spread of larval forms, direct inoculation after trauma, or reactivation of dormant intraocular cysts.
Parasites such as Toxocara canis, Onchocerca volvulus, Loa loa, Taenia solium (cysticercosis), and Toxoplasma gondii have all been implicated.
The disease is characterized by chronic granulomatous inflammation that can mimic uveitis, masquerade syndromes, or neoplastic processes, making diagnosis particularly challenging.
Pathophysiology
The underlying pathology is determined by the type of parasite and the host’s immune response. Parasites can reach the intraocular tissues through:
-
Hematogenous dissemination from systemic parasitic infection (e.g., toxocariasis, cysticercosis).
-
Direct inoculation following penetrating trauma or contaminated foreign bodies.
-
Local proliferation from intraocular cysts (e.g., ocular cysticercosis).
Once in the eye, parasites elicit a granulomatous inflammatory reaction, leading to:
-
Vitritis with dense membranes.
-
Retinochoroiditis with necrosis.
-
Intraocular granulomas or cysts.
-
Secondary complications such as retinal detachment, glaucoma, or phthisis bulbi.
The host immune response, while attempting to control the infection, often causes collateral tissue destruction and irreversible damage to ocular structures.
Epidemiology
Parasitic endophthalmitis is rare but has been reported globally, particularly in endemic regions:
-
Toxocara canis infections are more frequent in children with close contact to dogs.
-
Onchocerciasis and Loa loa filariasis are endemic in sub-Saharan Africa.
-
Cysticercosis is common in Latin America, Africa, and parts of Asia due to consumption of undercooked pork.
-
Immunocompromised individuals, including HIV/AIDS patients and transplant recipients, are at increased risk.
Although precise prevalence is difficult to determine, parasitic infections remain an important cause of intraocular inflammation in developing countries.

Clinical Features
The clinical presentation varies depending on the parasite and disease stage:
-
Acute symptoms: pain, photophobia, redness, blurred vision, floaters.
-
Ocular signs:
-
Anterior uveitis with hypopyon.
-
Vitritis with dense opacities.
-
Intraocular cysts or granulomas.
-
Retinal hemorrhages or necrosis.
-
Exudative retinal detachment.
-
-
Chronic course: gradual visual decline, persistent inflammation, or masquerade syndromes resembling intraocular tumors.
Examination Findings
-
Slit-lamp exam: corneal edema, keratic precipitates, anterior chamber cells, hypopyon.
-
Fundus exam: vitreous haze, white granulomas, retinal necrosis, localized traction.
-
B-scan ultrasonography: useful when media are opaque, showing vitreous membranes or intraocular cysts.
-
OCT (Optical Coherence Tomography): may demonstrate cystic structures or localized retinal damage.
Differential Diagnosis
Parasitic endophthalmitis must be differentiated from:
-
Bacterial or fungal endophthalmitis.
-
Chronic uveitis of autoimmune origin.
-
Ocular toxoplasmosis.
-
Intraocular lymphoma or retinoblastoma (in children).
-
Sarcoidosis or tuberculosis-related intraocular inflammation.
Diagnosis
A combination of clinical suspicion and laboratory investigations is essential:
-
Vitreous or aqueous tap: PCR for parasitic DNA.
-
Serology: ELISA for Toxocara, Toxoplasma, or cysticercosis.
-
Histopathology: demonstration of parasite or granulomatous reaction in enucleated specimens.
-
Imaging: orbital ultrasound, CT, or MRI to rule out extraocular cysts.
Management
Treatment requires a multimodal approach:
-
Antiparasitic therapy
-
Albendazole, ivermectin, and diethylcarbamazine (depending on parasite).
-
Corticosteroids are often added to reduce immune-mediated inflammation.
-
-
Surgical management
-
Pars plana vitrectomy for diagnostic purposes, cyst removal, or to clear vitreous opacities.
-
Enucleation may be necessary in painful blind eyes to control infection.
-
-
Supportive therapy
-
Management of complications such as glaucoma, retinal detachment, or cataract.
-
Prognosis
The visual prognosis of parasitic endophthalmitis is generally poor, especially when the diagnosis is delayed.
Early recognition and treatment can sometimes salvage useful vision, but in many cases, irreversible blindness occurs.
Enucleation may be required in severe, refractory disease. Preventive measures, including deworming programs, hygiene education, and safe food preparation, are essential in reducing disease burden.
Would you have interest in taking retinal images with your smartphone?
Fundus photography is superior to fundus analysis as it enables intraocular pathologies to be photo-captured and encrypted information to be shared with colleagues and patients.
Recent technologies allow smartphone-based attachments and integrated lens adaptors to transform the smartphone into a portable fundus camera and Retinal imaging by smartphone.
RETINAL IMAGING BY YOUR SMARTPHONE
References
-
Biswas J, et al. Parasitic infections of the eye: An overview. Indian J Med Microbiol. 2015;33(1):37–46.
-
Rathinam SR, et al. Ocular parasitic infections: Clinical aspects. Int Ophthalmol Clin. 2012;52(4):1–14.
-
Shields JA, Shields CL. Intraocular tumors: A text and atlas. Philadelphia: Lippincott Williams & Wilkins; 2008.
-
Khairallah M, et al. Ocular parasitic diseases: A review. Surv Ophthalmol. 2004;49(1):51–63.

{kind=link}