
Case Study
A 74-year-old woman with a history of untreated cataract in her right eye presented to the emergency department with severe ocular pain, redness, and markedly reduced vision for several days.

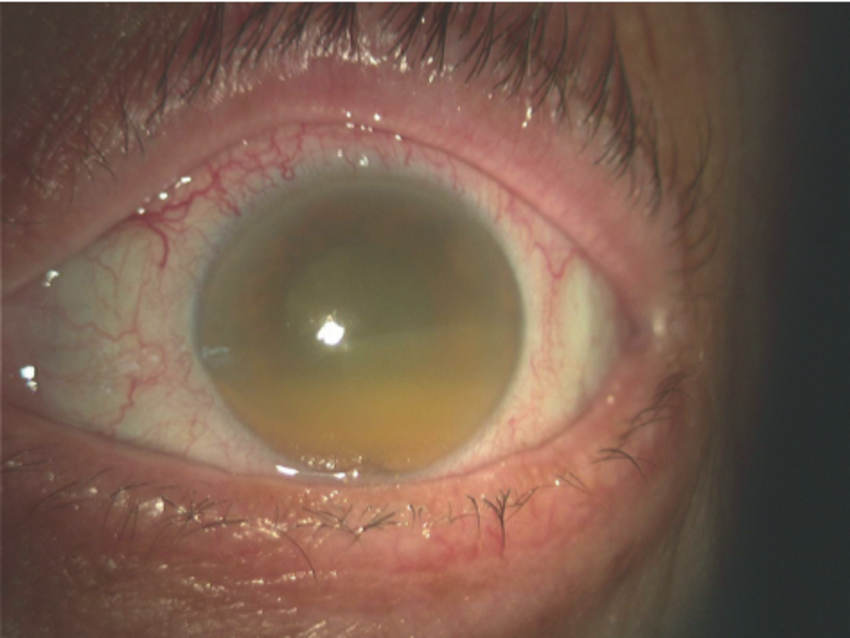
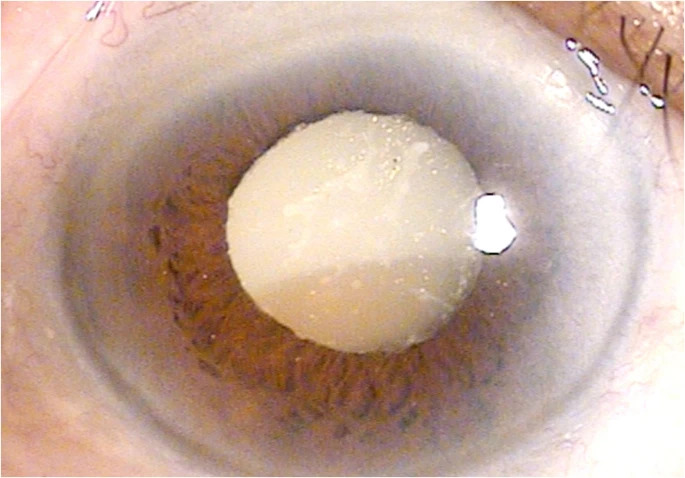
She reported halos around lights and nausea. On examination, visual acuity was counting fingers close to the face, intraocular pressure (IOP) measured 46 mmHg, and slit-lamp evaluation revealed a mature hypermature cataract with cortical material leaking into the anterior chamber.
Numerous macrophages engulfing lens proteins were visible as large cells floating in the aqueous humor. Corneal edema with microcystic changes and conjunctival congestion were also present.
The diagnosis of phacolytic glaucoma was made, and she underwent urgent management with IOP-lowering medications followed by cataract extraction, which resolved her symptoms.
Disease Entity
Phacolytic glaucoma is a secondary open-angle glaucoma that occurs due to leakage of high-molecular-weight lens proteins from a hypermature cataract into the anterior chamber.
The proteins attract macrophages, which obstruct the trabecular meshwork, causing aqueous outflow resistance and elevated IOP.
It typically presents in elderly patients with neglected cataracts and may mimic other causes of acute glaucoma.
Pathophysiology
In phacolytic glaucoma, the aging cataractous lens undergoes liquefaction, and capsule permeability increases, allowing lens proteins to escape into the aqueous humor.
These proteins act as antigens, eliciting an immune response that recruits macrophages. Engorged macrophages, together with free lens proteins, accumulate within the trabecular meshwork, obstructing aqueous outflow.
This blockage results in a rapid rise in IOP, corneal edema, and optic nerve damage if left untreated.
The inflammatory response can worsen trabecular dysfunction, and prolonged high IOP may cause permanent glaucomatous optic neuropathy.
Epidemiology
Phacolytic glaucoma is most commonly observed in patients over 70 years old, particularly in populations with limited access to cataract surgery.
With advancements in cataract extraction and early interventions, its prevalence has decreased in developed countries but remains an important cause of preventable vision loss in regions with limited healthcare access.
In many rural communities, the condition still accounts for a significant proportion of secondary glaucoma cases, highlighting disparities in healthcare delivery.
Clinical Features
Patients typically present with:
- Severe ocular pain and redness
- Decreased vision, often profound
- Halos around lights
- Headache, nausea, or vomiting due to elevated IOP
Examination Findings
- Visual acuity: severely reduced, often to hand movements or counting fingers
- IOP: markedly elevated, often >40 mmHg
- Slit-lamp: corneal edema, flare, cells, hypermature cataract, and macrophages in aqueous humor
- Gonioscopy: open angles with proteinaceous material and macrophages present
- Fundus: usually not visible due to corneal edema and cataract opacity; optic nerve assessment may require ultrasound or delayed evaluation after IOP control and cataract removal
Differential Diagnosis
- Phacomorphic glaucoma (due to lens-induced angle closure)
- Neovascular glaucoma (often secondary to ischemic retinal disease)
- Acute primary angle-closure glaucoma (typically without a mature cataract)
- Uveitic glaucoma (associated with anterior chamber reaction and synechiae)
Diagnosis
Diagnosis is made through clinical examination, focusing on the presence of a hypermature cataract, markedly elevated IOP, and macrophages in the anterior chamber.
Ancillary testing, such as ultrasound biomicroscopy, may be used to confirm the presence of cataractous changes in opaque corneas.
Aqueous humor aspiration can demonstrate lens proteins and phagocytic cells, supporting the diagnosis.
Management
- Medical management:
- Topical and systemic IOP-lowering agents (beta-blockers, alpha agonists, carbonic anhydrase inhibitors, hyperosmotic agents)
- Topical corticosteroids to reduce inflammation
- Cycloplegics to relieve pain and stabilize the blood-aqueous barrier
- Definitive treatment: extracapsular cataract extraction or phacoemulsification once IOP is controlled. In very advanced cases, manual small incision cataract surgery may be required due to lens density.
- Perioperative considerations: careful IOP control is critical before surgery to reduce the risk of expulsive hemorrhage. Postoperative glaucoma therapy may still be necessary if trabecular function does not fully recover.
Prognosis
With timely recognition and surgical intervention, the prognosis is favorable, and most patients recover functional vision.
However, delays in treatment can result in optic nerve damage, chronic secondary glaucoma, and permanent blindness.
Prognosis is poorer in patients presenting late, particularly if the optic nerve already shows glaucomatous cupping or if chronic high IOP has been longstanding.

Prevention
The best prevention is early cataract detection and surgical management before progression to the hypermature stage.
Public health strategies aimed at reducing barriers to cataract surgery—such as mobile eye units, surgical camps, and patient education—are essential in low-resource settings.
Patient counseling is crucial in convincing individuals with early cataracts not to delay surgery until vision is completely lost.
Conclusion
Phacolytic glaucoma remains an important cause of preventable blindness, particularly in underserved populations.
It highlights the critical need for early detection and timely management of cataracts.
Ophthalmologists should maintain a high index of suspicion in elderly patients presenting with acute glaucoma symptoms and a mature cataract, as prompt intervention can restore sight and prevent irreversible optic nerve damage.
HOW TO TAKE SLIT-LAMP EXAM IMAGES WITH A SMARTPHONE?
Smartphone slit-lamp photography is the new advancement in the field of science and technology in which photographs of the desired slit-lamp finding can be taken with smartphones by using the slit-lamp adapters.
Slit-lamp Smartphone photography
References
- Epstein DL, Jedziniak JA, Grant WM. Obstruction of aqueous outflow by lens particle and by heavy-molecular-weight soluble lens protein. Invest Ophthalmol Vis Sci. 1978.
- Shields MB. Textbook of Glaucoma. 6th ed. Lippincott Williams & Wilkins; 2011.
- Thomas R, et al. Phacolytic glaucoma: Pathogenesis and management. Ophthalmology Clinics. 1993.
- Ramakrishnan R, et al. Lens-induced glaucomas in the developing world: Epidemiology and risk factors. Curr Opin Ophthalmol. 2010.
- Thimons JJ, Gulati V. Lens-induced glaucoma. Glaucoma Today. 2012.

{kind=link}