
Case Study
A 60-year-old man with a 20-year history of gout and multiple tophaceous deposits in his extremities presented with worsening eye irritation, blurred vision, and halos around lights.

He had recently discontinued urate-lowering therapy due to poor compliance. On examination, slit-lamp evaluation revealed needle-shaped crystalline deposits in the corneal periphery and anterior chamber, along with conjunctival hyperemia and mild anterior uveitis.
Intraocular pressure was elevated at 28 mmHg, suggesting secondary glaucoma. Funduscopy showed no posterior segment involvement, but optical coherence tomography (OCT) revealed subtle irregularities in the corneal layers.
Laboratory tests confirmed serum uric acid levels of 11.2 mg/dL. The patient was diagnosed with ocular gout, and systemic as well as topical therapy was initiated to control inflammation and intraocular pressure.
Disease Entity
Ocular gout is an uncommon but clinically significant manifestation of systemic gout, defined by uric acid crystal deposition in various ocular structures.
While most cases of gout affect joints, tophaceous urate deposition in the eye can mimic other ophthalmic diseases, often leading to diagnostic delay.
Recognizing this rare entity is essential, as untreated cases can progress to vision-threatening complications.
Pathophysiology
Ocular gout arises from persistent hyperuricemia, resulting in supersaturation of monosodium urate and subsequent crystal deposition.
The eye is vulnerable due to avascular zones and fluid compartments where crystals can precipitate. Deposits are most frequently seen in:
- Cornea – stromal infiltration leading to opacification and visual impairment.
- Conjunctiva and sclera – chalky white nodules resembling subconjunctival tophi.
- Anterior chamber – free-floating or precipitated crystals, sometimes inducing anterior uveitis.
- Trabecular meshwork – blockage of aqueous humor outflow, causing secondary glaucoma.
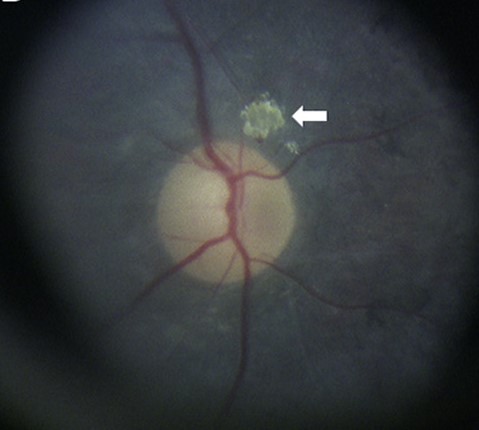
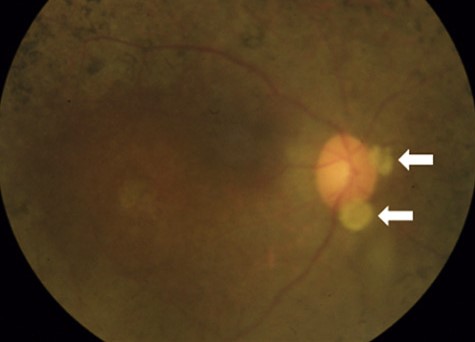
- Rare sites – retina, choroid, and lens, where deposits may compromise vascular supply or induce inflammatory changes.
Inflammation is driven by neutrophil activation, release of interleukin-1β, and oxidative stress, which together worsen ocular tissue damage.
Epidemiology
Although systemic gout affects 1–2% of adults in developed countries, ocular involvement remains rare and underreported.
It primarily affects men over 50 with longstanding uncontrolled gout, particularly those with visible tophaceous deposits.
The true prevalence may be underestimated due to a lack of awareness and misdiagnosis as uveitis, keratitis, or conjunctival lesions.
Clinical Features
Ocular gout may present with a spectrum of manifestations, including:
- Recurrent eye redness and irritation
- Foreign body sensation and photophobia
- Blurred vision or reduced visual acuity
- Halos around lights due to corneal edema
- Visible crystalline deposits in the conjunctiva, sclera, or cornea
- Signs of secondary glaucoma (elevated IOP, optic disc cupping)
- Anterior uveitis–like inflammation
Examination Findings
- Slit-lamp: white or needle-shaped crystalline deposits in cornea, conjunctiva, sclera, or anterior chamber
- Conjunctival tophi: chalky nodules, sometimes mimicking pinguecula
- IOP: often elevated due to trabecular obstruction
- Anterior chamber: inflammatory cells, flare, and crystals
- Posterior segment: usually spared, though rare reports describe retinal ischemia or urate deposition

Differential Diagnosis
- Band keratopathy
- Corneal dystrophies (lattice, granular)
- Calcific conjunctival deposits
- Ocular amyloidosis
- Chronic anterior uveitis of other etiologies
Diagnosis
Diagnosis relies on a combination of systemic history and ophthalmic examination. Supporting tools include:
- Serum uric acid measurement (typically elevated)
- Slit-lamp documentation of crystalline deposits
- Anterior segment OCT or confocal microscopy for crystal visualization
- Histopathological confirmation in excised lesions (rarely needed)
Management
Treatment of ocular gout requires systemic and local approaches:
- Systemic therapy: urate-lowering medications (allopurinol, febuxostat, uricosurics) and anti-inflammatory agents for acute gout attacks.
- Topical therapy: corticosteroid drops for inflammation, antiglaucoma medications if IOP is elevated.
- Surgical intervention: excision of conjunctival tophi or glaucoma surgery in refractory cases.
- Lifestyle modification: a diet low in purines, hydration, and avoidance of alcohol and certain medications.
Prognosis
The prognosis depends on early recognition and systemic control of hyperuricemia. With proper treatment, ocular deposits may regress, and inflammation subsides.
However, delayed diagnosis can lead to chronic keratopathy, persistent glaucoma, and irreversible visual loss.
Prevention
Preventive strategies include:
- Long-term urate-lowering therapy in patients with chronic gout
- Regular monitoring of serum uric acid
- Periodic ophthalmic screening in patients with severe tophaceous gout
- Patient education on adherence and lifestyle modification
Would you have interest in taking retinal images with your smartphone?
Fundus photography is superior to fundus analysis as it enables intraocular pathologies to be photo-captured and encrypted information to be shared with colleagues and patients.
Recent technologies allow smartphone-based attachments and integrated lens adaptors to transform the smartphone into a portable fundus camera and Retinal imaging by smartphone.
RETINAL IMAGING BY YOUR SMARTPHONE
References
- Fraunfelder FW. Ocular manifestations of gout. Am J Ophthalmol. 1990.
- Bhosle D, et al. Ocular urate deposits: A rare presentation of gout. Indian J Ophthalmol. 2014.
- Dalbeth N, et al. Pathophysiology of hyperuricemia and gout. Lancet. 2016.
- Kuo C, et al. Gout and the eye: A review. Surv Ophthalmol. 2020.

{kind=link}