
Case Study
A 68-year-old female presented with complaints of gradually worsening vision in both eyes over the past few years.

She reported increasing difficulty with reading, recognizing faces, and seeing at night, often noticing that lights had a noticeable glare.
The patient had a history of hypertension, which was well-controlled with medication, and no significant ocular history or previous eye surgeries.
Examination Results:
- Visual Acuity: 20/80 in both eyes.
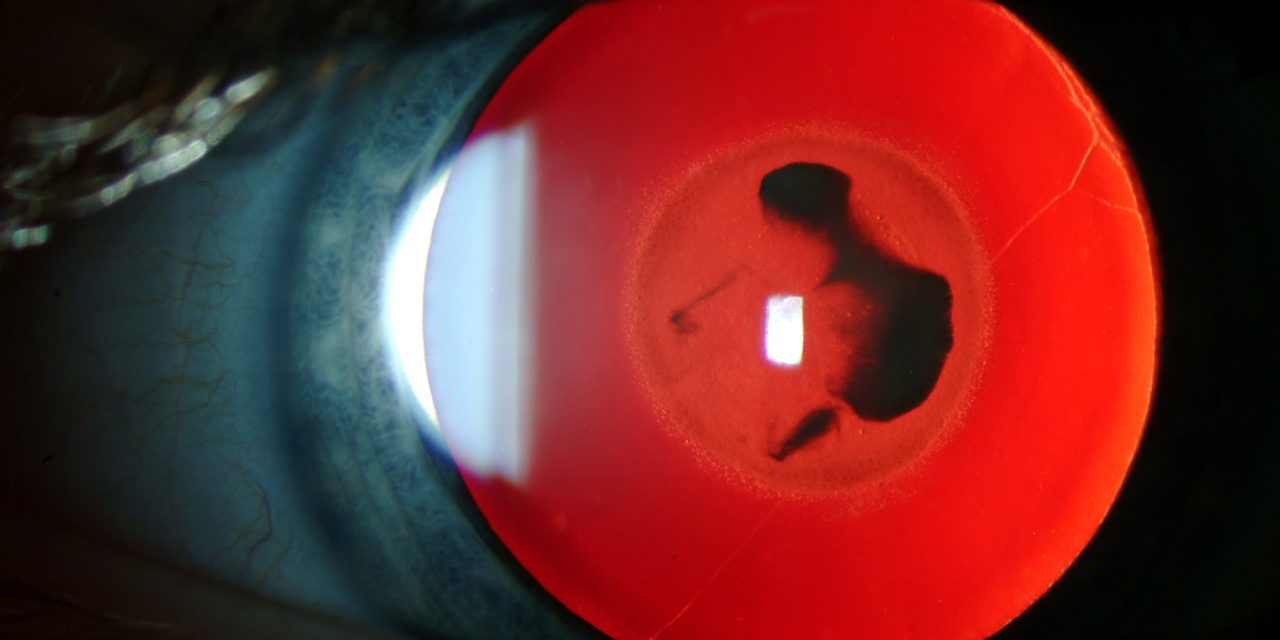
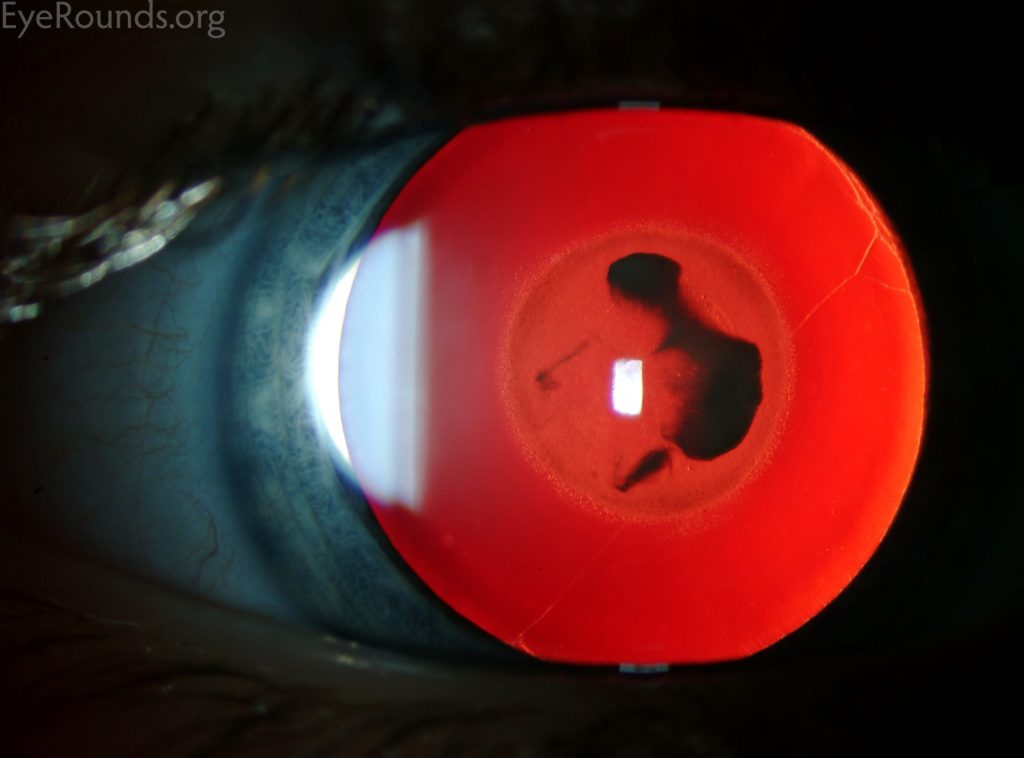
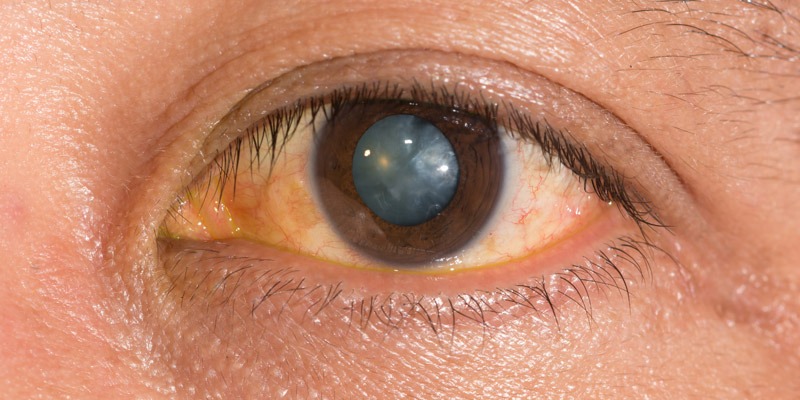
- Slit-Lamp Examination: Revealed a pronounced yellowing and opacification of the central portion of the lenses in both eyes, characteristic of nuclear cataract.
- Fundus Examination: Limited view due to the cataracts, but no significant retinal abnormalities were visible.
- Intraocular Pressure (IOP): 15 mmHg in both eyes.
The patient was diagnosed with Bilateral Nuclear Cataract.
Nuclear Cataract entity
Nuclear Cataract is a type of age-related cataract that specifically affects the central part of the lens, known as the nucleus.
This condition is the most common form of cataract, particularly in older adults. It develops slowly and can significantly impact vision over time, making everyday tasks such as reading and driving increasingly difficult.
The gradual hardening and yellowing of the lens nucleus lead to a progressive decline in visual clarity, often affecting both near and distant vision.
Nuclear Cataracts are associated with the natural aging process, although certain risk factors such as smoking, excessive sun exposure, and long-term use of corticosteroids can accelerate their development.
The condition is typically bilateral, with both eyes being affected, although the severity may vary between the eyes.
Nuclear cataracts not only reduce visual acuity but also alter color perception, making colors appear dull and less vibrant.
Pathophysiology
The pathophysiology of nuclear cataracts involves the gradual accumulation of oxidative damage and protein aggregation in the lens nucleus, leading to increased lens density and opacification.
The lens nucleus, composed of older lens fibers, is particularly susceptible to age-related changes due to its limited capacity for cellular repair and renewal.
Over time, continuous exposure to oxidative stress, ultraviolet (UV) light, and other environmental factors contributes to the formation of yellow-brown pigments, known as chromophores, within the lens.
These chromophores not only reduce the transparency of the lens but also alter its refractive properties, often resulting in a shift towards myopia (nearsightedness).
This phenomenon, known as “second sight,” may temporarily improve near vision in presbyopic individuals but ultimately worsens as the cataract progresses.
The nuclear sclerosis and hardening of the lens nucleus further contribute to light scattering, glare, and reduced contrast sensitivity, significantly impairing visual function.
Epidemiology
Nuclear cataracts are the most common type of age-related cataracts, particularly in individuals over the age of 65.
The prevalence of nuclear cataracts increases with age, with nearly half of all people over the age of 75 having some degree of nuclear lens opacification.
The condition affects both men and women, although some studies suggest a slightly higher prevalence in women.
Risk factors for nuclear cataracts include:
- Aging: The primary risk factor, as nuclear cataracts are strongly associated with the natural aging process.
- Genetic Predisposition: A family history of cataracts may increase the likelihood of developing nuclear cataracts.
- Smoking: Long-term smoking is a well-documented risk factor, likely due to increased oxidative stress on the lens.
- Ultraviolet (UV) Light Exposure: Prolonged exposure to UV radiation from sunlight contributes to the development of nuclear cataracts.
- Chronic Disease: Conditions such as diabetes and hypertension have been associated with an increased risk of nuclear cataracts.
- Corticosteroid Use: Long-term use of corticosteroids is linked to a higher incidence of cataract formation, including nuclear cataracts.

Nuclear Cataract Clinical Features
Nuclear cataracts present with a range of symptoms that progressively worsen over time. The most common clinical features include:
- Blurry Vision: A gradual decline in visual acuity, particularly in low light conditions or at night.
- Myopic Shift: A noticeable increase in nearsightedness, often referred to as “second sight,” where patients may temporarily find that their near vision improves.
- Difficulty with Color Perception: Colors may appear less vibrant, with whites taking on a yellowish hue.
- Glare and Halos: Increased sensitivity to bright lights, often resulting in glare and halos around light sources, especially at night.
- Difficulty with Reading and Fine Detail: As the cataract progresses, patients may find it challenging to read small print or perform tasks that require fine visual detail.
Examination Findings
- Slit-Lamp Examination: The hallmark finding in nuclear cataracts is the yellowing and opacification of the lens nucleus, visible as increased density and sclerosis of the central lens. In advanced cases, the lens may appear brown or brunescent.
- Fundus Examination: Visualization of the retina may be impaired due to lens opacity, but the fundus may appear normal if no other ocular conditions are present.
- Visual Acuity Testing: Typically reveals a gradual decline in distance vision, with possible improvement in near vision due to myopic shift.
- Intraocular Pressure (IOP): Generally normal, but regular monitoring is essential to rule out secondary glaucoma.
Differential Diagnosis
The differential diagnosis of nuclear cataract includes other forms of cataract and ocular conditions that cause similar visual disturbances:
- Cortical Cataract: Characterized by spoke-like opacities in the lens cortex, often causing glare and difficulty with night vision.
- Posterior Subcapsular Cataract (PSC): Affects the back of the lens, often leading to glare and difficulty with near vision.
- Age-related macular Degeneration (AMD): May cause central vision loss and should be differentiated from cataract-related vision impairment.
- Diabetic Retinopathy: Can present with visual disturbances due to retinal changes and should be considered in diabetic patients.
- Keratoconus: A progressive thinning and cone-like protrusion of the cornea, leading to visual distortion.
Nuclear CataractDiagnosis
Diagnosis of nuclear cataract is based on clinical evaluation and imaging:
- Slit-Lamp Examination: Essential for visualizing the lens nucleus and assessing the extent of cataract formation.
- Visual Acuity Testing: Provides insight into the impact of the cataract on the patient’s vision.
- Dilated Fundus Examination: Important for ruling out other retinal or optic nerve conditions that may contribute to visual impairment.
- Optical Coherence Tomography (OCT): This may be used to assess the retina if fundus examination is difficult due to lens opacity.
Nuclear Cataract Management
Management of nuclear cataracts primarily involves surgical intervention, particularly when the cataract significantly impairs the patient’s quality of life:
- Cataract Surgery: The definitive treatment for nuclear cataracts is phacoemulsification with intraocular lens (IOL) implantation. This procedure involves the removal of the opacified lens nucleus and its replacement with a clear artificial lens. Surgery is typically recommended when the cataract interferes with daily activities such as reading, driving, or recognizing faces.
- Preoperative Evaluation: A thorough evaluation, including measurements for IOL power calculation, is necessary to ensure optimal surgical outcomes.
- Postoperative Care: Involves the use of anti-inflammatory and antibiotic eye drops to prevent infection and promote healing. Regular follow-up is essential to monitor the surgical site and assess visual recovery.
- Visual Rehabilitation: Following surgery, patients may require glasses or contact lenses for optimal vision correction, particularly if a monofocal IOL is used.
![]()
Prognosis
The prognosis for patients with nuclear cataracts is generally excellent following cataract surgery. Most patients experience a significant improvement in visual acuity and quality of life.
However, the outcome depends on the presence of any coexisting ocular conditions, such as age-related macular degeneration or diabetic retinopathy, which may limit visual recovery.
Early intervention and appropriate management of systemic risk factors can help prevent the progression of cataracts and improve surgical outcomes.
Nuclear Cataract Prevention
While nuclear cataract is primarily an age-related condition, certain lifestyle modifications can reduce the risk or delay the onset of cataract formation:
- Smoking Cessation: Quitting smoking can reduce the risk of cataract development.
- UV Protection: Wearing sunglasses with UV protection can help protect the eyes from harmful radiation and reduce the risk of cataract formation.
- Diet and Nutrition: A diet rich in antioxidants, such as vitamins C and E, may help protect the lens from oxidative damage.
- Regular Eye Examinations: Routine eye exams are essential for early detection and management of cataracts, particularly in individuals over the age of 50.
HOW TO TAKE SLIT-LAMP EXAM IMAGES WITH A SMARTPHONE?
Smartphone slit-lamp photography is the new advancement in the field of science and technology in which photographs of the desired slit-lamp finding can be taken with smartphones by using the slit-lamp adapters.
Slit-lamp Smartphone photography
References
- Asbell, P. A., Dualan, I., Mindel, J., Brocks, D., Ahmad, M., & Epstein, S. (2005). Age-related cataract. The Lancet, 365(9459), 599-609.
- Congdon, N., Vingerling, J. R., Klein, B. E., West, S., Friedman, D. S., Kempen, J., … & Taylor, H. R. (2004). Prevalence of cataract and pseudophakia/aphakia among adults in the United States. Archives of Ophthalmology, 122(4), 487-494.
- West, S. K., & Valmadrid, C. T. (1995). Epidemiology of risk factors for age-related cataract. Survey of Ophthalmology, 39(4), 323-334.
- Thylefors, B., & Negrel, A. D. (1994). The global impact of cataract blindness. Bulletin of the World Health Organization, 72(2), 323-326.
- Bollinger, K. E., & Langston, R. H. (2008). What can patients expect from cataract surgery? Cleveland Clinic Journal of Medicine, 75(3), 193-200.
- Cumming, R. G., Mitchell, P., & Leeder, S. R. (1997). Use of inhaled corticosteroids and the risk of cataracts. New England Journal of Medicine, 337(1), 8-14.

{kind=link}