

Case Study
A 28-year-old male presented to the ophthalmology clinic with complaints of sudden-onset redness, eye pain, photophobia, and blurry vision in his right eye for the past three days.


He denied any history of trauma, ocular surgery, or systemic illness. On examination, visual acuity in the right eye was 6/9.
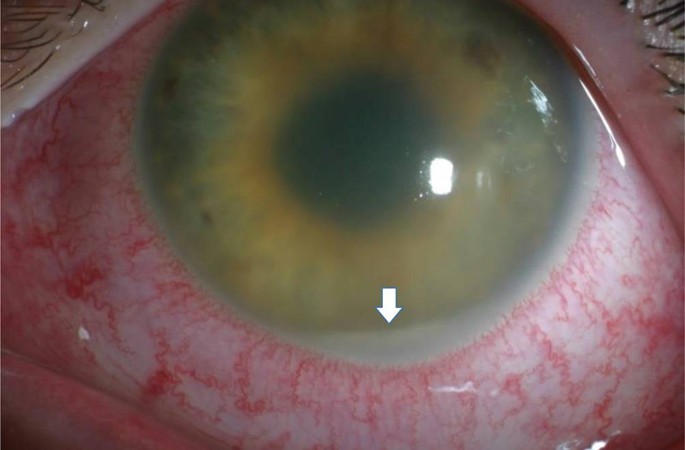
Slit-lamp examination showed ciliary injection, 2+ anterior chamber cells and flare, fine non-granulomatous keratic precipitates, and an irregularly shaped pupil suggestive of posterior synechiae.
Intraocular pressure was 10 mmHg. Fundus examination was normal. A diagnosis of Acute Anterior Uveitis (AAU) was made.
Further workup revealed HLA-B27 positivity, and a referral to rheumatology confirmed undiagnosed ankylosing spondylitis.
Disease Entity
Acute Anterior Uveitis (AAU) is the most common form of intraocular inflammation, characterized by the sudden onset of inflammation predominantly confined to the anterior segment of the eye.
It typically affects the iris and ciliary body and is considered a type of anterior uveitis, which accounts for 50–90% of all uveitis cases.
The disease may present in isolation or in association with systemic inflammatory conditions, most notably HLA-B27-associated spondyloarthropathies.
Pathophysiology
The underlying mechanism of AAU involves breakdown of the blood-aqueous barrier, allowing infiltration of leukocytes and inflammatory mediators into the anterior chamber.
This process may be triggered by:
-
Autoimmune mechanisms, particularly in HLA-B27-positive individuals
-
Infectious agents, such as herpes simplex virus or tuberculosis
-
Post-traumatic causes, such as blunt injury or surgical procedures
-
Idiopathic causes, when no underlying etiology is identified
The hallmark features include T-cell–mediated immune responses and overproduction of cytokines such as TNF-α, IL-6, and IFN-γ, which drive local inflammation, resulting in pain, photophobia, and anterior chamber reaction.
Epidemiology
-
Most common in adults aged 20–50 years
-
Slight male predominance, especially in HLA-B27-associated cases
-
Higher prevalence in Caucasian populations
-
Accounts for up to 90% of uveitis cases in tertiary care centers
-
Frequently recurrent, with episodes varying in severity and duration
-
Associated systemic conditions:
-
Ankylosing spondylitis
-
Reactive arthritis
-
Psoriatic arthritis
-
Inflammatory bowel disease
-
Juvenile idiopathic arthritis (in children)
-
Clinical Features
-
Unilateral involvement is typical
-
Sudden onset
-
Redness, often sectoral with ciliary flush
-
Photophobia and pain
-
Blurry vision
-
Tearing or epiphora
-
Mild ptosis in some cases
Systemic symptoms, such as joint pain or back stiffness, may be present in those with associated autoimmune disorders.
Examination Findings
On slit-lamp examination:
-
Ciliary injection (perilimbal redness)
-
Anterior chamber cells and flare
-
Keratic precipitates (KPs): typically fine and non-granulomatous
-
Posterior synechiae: iris adhesions to the lens
-
Hypopyon: leukocyte layering in severe inflammation
-
Small, irregular pupil due to iris sphincter spasm
-
Iris nodules in granulomatous variants
-
Low intraocular pressure early in the disease
-
Elevated IOP later in steroid responders or trabeculitis
Differential Diagnosis
-
Herpetic anterior uveitis
-
Fuchs heterochromic iridocyclitis
-
Sarcoid uveitis
-
Tuberculous uveitis
-
Juvenile idiopathic arthritis–associated uveitis
-
Masquerade syndromes (e.g., intraocular lymphoma)
-
Post-traumatic iritis
Diagnosis
AAU is a clinical diagnosis supported by history and examination. Investigations are directed by clinical suspicion.
Baseline tests may include:
-
HLA-B27 typing
-
ESR, CRP (inflammatory markers)
-
ANA, RF (in suspected autoimmune diseases)
-
VDRL/FTA-ABS (for syphilis)
-
PPD or IGRA (for TB)
-
ACE, chest X-ray (for sarcoidosis)
-
PCR testing (in suspected viral cases)
Imaging:
-
Sacroiliac joint X-ray or MRI in suspected spondyloarthropathy
-
Anterior segment OCT or UBM in atypical presentations
Management
Topical Treatment
-
Corticosteroids (e.g., prednisolone acetate 1%): the mainstay of treatment, started intensively and tapered as inflammation subsides
-
Cycloplegic agents (e.g., homatropine, atropine): relieve pain and prevent posterior synechiae
Systemic Treatment
-
Oral corticosteroids in severe or refractory cases
-
Immunosuppressive therapy for chronic, bilateral, or systemic-associated disease (methotrexate, cyclosporine, TNF-α inhibitors)
Infectious AAU
-
Requires specific antimicrobial therapy in addition to corticosteroids
-
Herpetic uveitis: acyclovir or valacyclovir
Monitoring
-
Regular follow-up to monitor intraocular pressure and response to therapy
-
Fundus examination to rule out posterior involvement
-
Rheumatology or infectious disease referral when systemic association is suspected
Prognosis
-
Prognosis is generally good with appropriate and timely treatment
-
Visual recovery is expected in most cases
-
Recurrence is common in HLA-B27-associated cases
-
Potential complications if not treated:
-
Posterior synechiae
-
Cataract
-
Secondary glaucoma
-
Cystoid macular edema
-
Band keratopathy
-

Prevention
-
No specific prevention for idiopathic AAU
-
Early diagnosis and management of associated systemic diseases can reduce recurrence
-
Long-term follow-up in recurrent or chronic cases
-
Patient education on early symptoms (pain, redness, photophobia) to encourage early presentation
Conclusion
Acute Anterior Uveitis is a common, treatable form of ocular inflammation that often serves as a window to underlying systemic disease.
A detailed history, comprehensive slit-lamp examination, and targeted investigations help guide appropriate treatment.
Collaboration with rheumatologists and infectious disease specialists ensures optimal outcomes, especially in recurrent or complicated cases.
With prompt management, the prognosis is favorable, but vigilance is key to preventing long-term complications.
HOW TO TAKE SLIT-LAMP EXAM IMAGES WITH A SMARTPHONE?
Smartphone slit-lamp photography is the new advancement in the field of science and technology in which photographs of the desired slit-lamp finding can be taken with smartphones by using the slit-lamp adapters.
Slit-lamp Smartphone photography
References
-
Jabs DA, Nussenblatt RB, Rosenbaum JT. Standardization of Uveitis Nomenclature for Reporting Clinical Data. Am J Ophthalmol. 2005.
-
Rosenbaum JT, Bodaghi B, Couto C, Zierhut M. Uveitis: Etiology and Approach to Diagnosis. Duane’s Ophthalmology.
-
Gritz DC, Wong IG. Incidence and Prevalence of Uveitis in Northern California: The Northern California Epidemiology of Uveitis Study. Ophthalmology. 2004.
-
Foster CS, Vitale AT. Diagnosis and Treatment of Uveitis. WB Saunders; 2002.
-
Smith JR, Rosenbaum JT. Management of uveitis: a rheumatologic perspective. Arthritis Rheum. 2002.

{kind=link}