

Case Study
A 42-year-old male presented to the ophthalmology clinic complaining of progressive vision loss, photophobia, and occasional pain in his right eye over the past six months.


The patient reported a history of ocular trauma caused by a metallic fragment while welding two years earlier. On examination, visual acuity was 20/200 in the affected eye and 20/20 in the fellow eye.
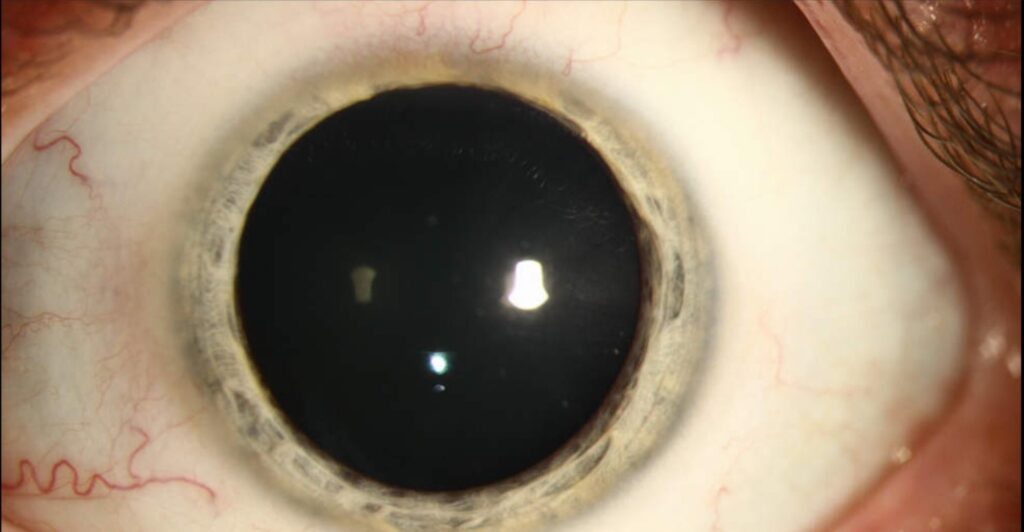
The cornea showed subtle brownish discoloration, the iris appeared heterochromic with rusty pigmentation, and the pupil reaction was sluggish.
Fundus examination revealed a diffuse brownish hue, attenuation of retinal vessels, and evidence of retinal pigment epithelium (RPE) degeneration.
Electroretinography (ERG) demonstrated markedly reduced amplitudes, suggesting retinal toxicity. Ultrasonography identified a small metallic intraocular foreign body embedded in the peripheral retina.
The diagnosis of siderosis bulbi was made, and prompt surgical removal of the foreign body was performed to prevent further ocular damage.
Introduction
Siderosis bulbi is a toxic condition of the eye caused by prolonged intraocular retention of an iron-containing foreign body.
The term “siderosis” refers to the deposition of iron in ocular tissues, leading to progressive structural and functional damage.
Although rare in modern ophthalmology due to improved imaging and early foreign body detection, it remains an important cause of delayed visual loss following penetrating ocular injury.
The condition is insidious, with symptoms often appearing months or years after the initial trauma, making timely recognition and management crucial for preserving vision.
Pathophysiology
Iron from an intraocular foreign body gradually dissolves into ocular fluids and is transported into various ocular tissues.
This leads to the formation of ferritin and hemosiderin, which accumulate in the cornea, iris, lens, retina, and ciliary body.
The deposited iron catalyzes oxidative stress, damaging cell membranes and mitochondria, particularly in metabolically active tissues such as the retina.
Photoreceptor cells and RPE are especially susceptible to iron toxicity, resulting in progressive degeneration and functional impairment, detectable through electroretinography (ERG).
Over time, the continued deposition of iron leads to irreversible structural changes, including corneal endothelial damage, cataract formation, and retinal atrophy.
Epidemiology
Siderosis bulbi most commonly affects young males, as they are more prone to occupational ocular injuries involving metallic fragments, such as welding, grinding, or hammering.
The time between injury and clinical manifestation may vary from months to several years, depending on the size, composition, and location of the intraocular foreign body.
Iron-containing ferromagnetic materials pose the highest risk, while inert metals such as copper alloys or aluminum rarely cause siderosis.
With increased use of protective eyewear and early diagnostic imaging, the incidence of this condition has significantly declined in recent decades.

Clinical Features
The clinical manifestations of siderosis bulbi are diverse and depend on the location and extent of iron deposition. Common findings include:
-
Cornea: Rust-colored discoloration of the epithelium and endothelium, with possible development of band keratopathy.
-
Iris: Heterochromia (the affected iris becomes brownish or rust-colored), mydriasis, and reduced pupillary reactions due to sphincter paralysis.
-
Lens: Formation of a characteristic brownish anterior subcapsular cataract known as a “siderotic cataract.”
-
Retina: Attenuation of retinal vessels, RPE mottling, and pigmentary degeneration resembling retinitis pigmentosa.
-
Electroretinography (ERG): Early functional impairment is reflected in decreased a- and b-wave amplitudes, even before visible retinal damage occurs.
Patients may initially experience photophobia, blurred vision, or nyctalopia, which can progress to severe vision loss if the foreign body remains unremoved.
Diagnosis
Diagnosis of siderosis bulbi relies on a detailed history, clinical examination, and imaging studies to detect the intraocular foreign body and assess the extent of damage.
-
Slit-lamp examination: Reveals characteristic rust-colored deposits and pigmentary changes in the anterior segment.
-
Fundus examination: Shows diffuse brownish discoloration, vessel attenuation, and RPE changes.
-
Ultrasound B-scan: Useful for detecting metallic foreign bodies when direct visualization is not possible due to media opacity.
-
CT Scan (Orbit): The preferred imaging modality to localize metallic intraocular foreign bodies and differentiate them from non-metallic materials.
-
Electroretinography (ERG): A sensitive test that detects early functional retinal impairment before structural damage occurs.
-
Anterior Segment Optical Coherence Tomography (AS-OCT) and Ultrasound Biomicroscopy (UBM): Help assess the location of anterior segment foreign bodies.
Differential Diagnosis
Conditions that may mimic siderosis bulbi include:
-
Chalcosis bulbi (copper toxicity)
-
Pigmentary glaucoma
-
Retinitis pigmentosa
-
Chronic uveitis
-
Post-traumatic cataract
Management
The cornerstone of treatment for siderosis bulbi is early identification and removal of the intraocular foreign body.
The prognosis depends on the duration of iron exposure and the extent of ocular tissue damage at the time of intervention.
-
Surgical removal: The foreign body is extracted via pars plana vitrectomy, depending on its location and accessibility.
-
Medical management: While chelating agents such as deferoxamine have been explored, they have limited efficacy in reversing established ocular siderosis.
-
Supportive care: Includes management of secondary complications such as cataract extraction, control of secondary glaucoma, and low-vision rehabilitation if vision loss is irreversible.
Postoperative follow-up is essential to monitor for delayed toxicity or residual foreign body fragments. Electroretinography may be repeated periodically to assess the functional recovery of the retina.
Prognosis
Visual outcome depends on the duration of exposure before removal of the foreign body. If the metallic fragment is removed promptly, some degree of retinal function can be preserved, and progression of toxicity may halt.
However, delayed diagnosis often results in irreversible retinal damage, optic atrophy, and permanent vision loss.
Prevention
Prevention of siderosis bulbi primarily involves proper eye protection during high-risk activities such as welding, metal grinding, and industrial work.
Early ophthalmic evaluation following any ocular trauma is essential, even if symptoms appear minimal.
Educating patients about the long-term risks of retained intraocular foreign bodies can prevent this devastating but avoidable complication.
HOW TO TAKE SLIT-LAMP EXAM IMAGES WITH A SMARTPHONE?
Smartphone slit-lamp photography is the new advancement in the field of science and technology in which photographs of the desired slit-lamp finding can be taken with smartphones by using the slit-lamp adapters.
Slit-lamp Smartphone photography
References
-
Hope-Ross MW, Mahon GJ, Johnston PB. Ocular siderosis. Eye (Lond). 1993;7(Pt 3):419–425.
-
Bains HS, Mohan S, Gupta A. Siderosis bulbi: clinical presentation, pathogenesis and management. Indian J Ophthalmol. 2020;68(7):1381–1388.
-
Bains HS, Gupta A, et al. Evaluation of retinal function using ERG in ocular siderosis. Br J Ophthalmol. 2014;98(7):911–915.
-
Hope-Ross MW, et al. The role of imaging in the diagnosis and management of intraocular foreign bodies. Surv Ophthalmol. 1993;37(1):1–34.

{kind=link}