
Case study
A 28-year-old female presented to an ophthalmology clinic with complaints of sudden onset blurred vision and scotomas in both eyes over the past two days.


She described the visual disturbances as central dark spots and noted difficulty in reading and recognizing faces. The patient denied any pain or photophobia.
She had no significant medical history but reported a recent upper respiratory tract infection.
Examination Results:
- Visual Acuity: 20/40 in both eyes.
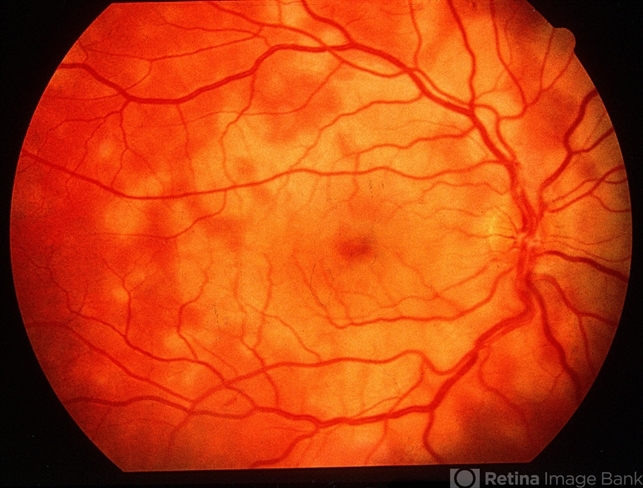
- Fundus Examination: Multiple yellow-white placoid lesions at the level of the retinal pigment epithelium (RPE) in the posterior pole of both eyes.
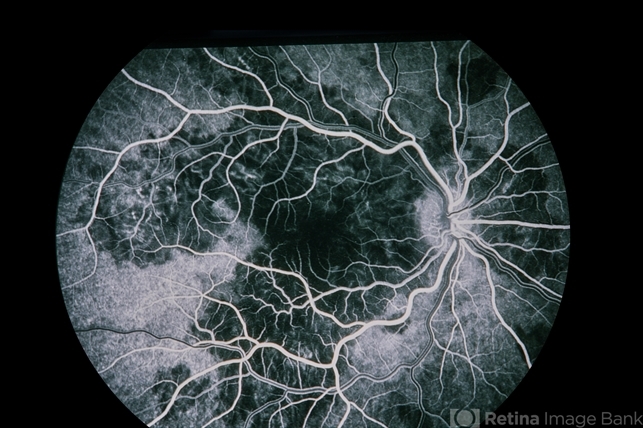
- Fluorescein Angiography: Early hypofluorescence of the lesions with late staining.
- Optical Coherence Tomography (OCT): Disruption of the outer retinal layers, including the ellipsoid zone and RPE, with areas of subretinal fluid.
- Indocyanine Green Angiography (ICG): Hypofluorescent spots corresponding to areas of choriocapillaris non-perfusion.
- Systemic Workup: Normal results, ruling out infectious or systemic inflammatory diseases.
Acute Posterior Multifocal Placoid Pigment Epitheliopathy (APMPPE) diagnosis was confirmed.
Disease entity
Acute Posterior Multifocal Placoid Pigment Epitheliopathy (APMPPE) is a rare inflammatory condition affecting the retinal pigment epithelium (RPE) and outer retina.
First described by Donald Gass in 1968, APMPPE typically presents with sudden, painless vision loss or visual disturbances in one or both eyes.
The etiology remains unclear, but it is thought to involve an inflammatory or autoimmune process.
Pathophysiology
The exact cause of APMPPE is unknown, but it is believed to involve an immune-mediated response.
The condition may be triggered by a viral or bacterial infection, leading to inflammation and subsequent damage to the RPE and choriocapillaris.
The inflammation results in the characteristic placoid lesions seen in APMPPE.
Histopathological studies suggest that the primary site of damage is the choriocapillaris, with secondary involvement of the RPE and outer retina.
This ischemic damage leads to the disruption of the outer blood-retinal barrier, causing fluid accumulation and retinal detachment in the affected areas.
Epidemiology
APMPPE primarily affects young adults, with a slight male predominance. The age of onset is typically between 20 and 40 years, but cases have been reported in children and older adults.
The incidence of APMPPE is low, and it is considered a rare condition. There is no significant racial or geographic predilection.
Clinical Features
Patients with APMPPE usually present with the following symptoms:
- Sudden Vision Loss: Rapid onset of blurred vision or central scotomas (blind spots) in one or both eyes.
- Photopsia: Flashing lights or flickering in the visual field.
- Metamorphopsia: Distorted vision, where straight lines appear wavy or bent.
- Mild Ocular Discomfort: Although the condition is typically painless, some patients may experience mild eye discomfort or headache.
Examination Findings
- Fundus Examination: Multiple, yellow-white placoid lesions at the level of the RPE, primarily affecting the posterior pole. These lesions may be confluent or discrete and often involve the macula.
- Fluorescein Angiography: Early hypofluorescence of the placoid lesions due to blockage of choroidal fluorescence, followed by late hyperfluorescence as the lesions stain.
- Optical Coherence Tomography (OCT): Disruption of the outer retinal layers, including the ellipsoid zone and RPE, with areas of subretinal fluid and retinal thickening.
- Indocyanine Green Angiography (ICG): Hypofluorescent spots corresponding to areas of choriocapillaris non-perfusion.
Differential Diagnosis
Several other conditions can present with similar symptoms and clinical findings, necessitating a thorough differential diagnosis:
- Serpiginous Choroidopathy: Characterized by slowly progressive, serpentine-shaped lesions involving the RPE and choriocapillaris.
- Multiple Evanescent White Dot Syndrome (MEWDS): Typically affects young women and presents with multiple small, white dots at the level of the RPE, often accompanied by photopsia and an enlarged blind spot.
- Birdshot Chorioretinopathy: Presents with multiple cream-colored lesions at the level of the choroid and RPE, often associated with vitritis.
- Viral Retinitis: Conditions such as acute retinal necrosis (ARN) and cytomegalovirus (CMV) retinitis can present with similar fundus findings but are usually accompanied by significant intraocular inflammation.
- Sarcoidosis: Can cause granulomatous inflammation of the choroid and retina, leading to multifocal chorioretinal lesions.

Diagnosis
Diagnosing APMPPE involves a combination of clinical evaluation, imaging studies, and exclusion of other conditions:
- Clinical Examination: Thorough fundus examination to identify characteristic placoid lesions.
- Fluorescein Angiography: Essential for demonstrating the early hypofluorescence and late hyperfluorescence of the lesions.
- Optical Coherence Tomography (OCT): Provides detailed cross-sectional imaging of the retina, highlighting disruptions in the outer retinal layers.
- Indocyanine Green Angiography (ICG): Useful for assessing choroidal involvement and non-perfusion areas.
- Systemic Evaluation: To rule out underlying systemic inflammatory or infectious conditions, including laboratory tests and imaging studies as needed.
Management
The management of APMPPE is primarily supportive, as the condition is often self-limiting:
- Observation: Many cases of APMPPE resolve spontaneously within weeks to months, with gradual improvement in vision.
- Corticosteroids: Systemic corticosteroids may be considered in severe or bilateral cases to reduce inflammation and expedite recovery.
- Immunosuppressive Therapy: In refractory cases or those with associated systemic inflammatory conditions, immunosuppressive agents such as azathioprine or mycophenolate mofetil may be used.
- Monitoring: Regular follow-up to monitor the resolution of lesions and recovery of visual function, as well as to detect any complications.
Prognosis
The prognosis for patients with APMPPE is generally favorable, with most patients experiencing significant improvement in vision over time.
However, some patients may have residual visual deficits, such as persistent scotomas or mild metamorphopsia. Recurrences are rare but can occur, necessitating long-term follow-up.
Prevention
There are no specific preventive measures for APMPPE, given its unclear etiology. Public health efforts should focus on raising awareness among healthcare providers and the general population to ensure timely diagnosis and management.
Increased awareness can lead to earlier intervention, reducing the risk of complications and improving patient outcomes.
Would you have interest in taking retinal images with your smartphone?
Fundus photography is superior to fundus analysis as it enables intraocular pathologies to be photo-captured and encrypted information to be shared with colleagues and patients.
Recent technologies allow smartphone-based attachments and integrated lens adaptors to transform the smartphone into a portable fundus camera and Retinal imaging by smartphone.
RETINAL IMAGING BY YOUR SMARTPHONE
References
- Gass, J. D. M. (1968). Acute Posterior Multifocal Placoid Pigment Epitheliopathy. Archives of Ophthalmology, 80(2), 177-185.
- Fiore, T., & Iaccheri, B. (2009). Acute posterior multifocal placoid pigment epitheliopathy: current perspectives. Clinical Ophthalmology (Auckland, N.Z.), 3, 503-507.
- Bouchenaki, N., & Cimino, L. (2000). Acute posterior multifocal placoid pigment epitheliopathy: a choroidal ischaemic disease. Graefe’s Archive for Clinical and Experimental Ophthalmology, 238(10), 912-917.
- Wolf, M. D., & Folk, J. C. (1991). Long-term visual function in acute posterior multifocal placoid pigment epitheliopathy. Archives of Ophthalmology, 109(6), 800-803.
- Ryan, S. J. (2006). Retina (4th ed.). Elsevier Health Sciences.

{kind=link}