
CASE REPORT
A 66-year-old male presented with 2 weeks of right eye pain, redness, and a nasal visual field defect. Past ocular history was significant for cataract surgery in the left eye.

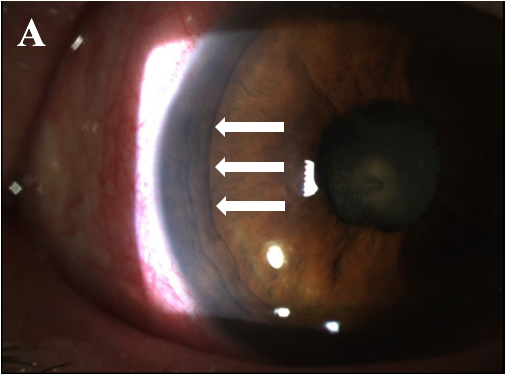
He had no history of previous trauma and was systemically healthy. Examination revealed a visual acuity of 20/400, ciliary flush, and iris heterochromia with a green right iris compared to a blue left iris.
Posterior synechiae were present at 360° in the right eye. Intraocular pressure (IOP) was 6 mm Hg in the right and 17 mm Hg in the left.
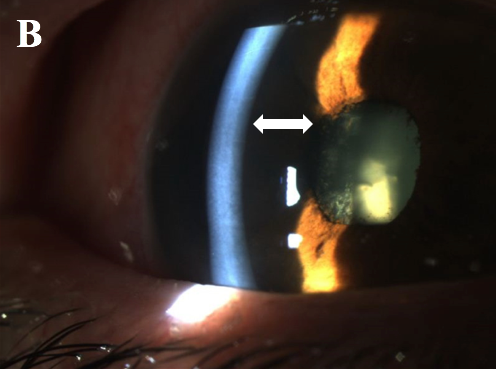
Gonioscopy and Slit lamp examination demonstrated a very deep right anterior chamber with inferior posterior synechiae, 2+ flare, and no cell.
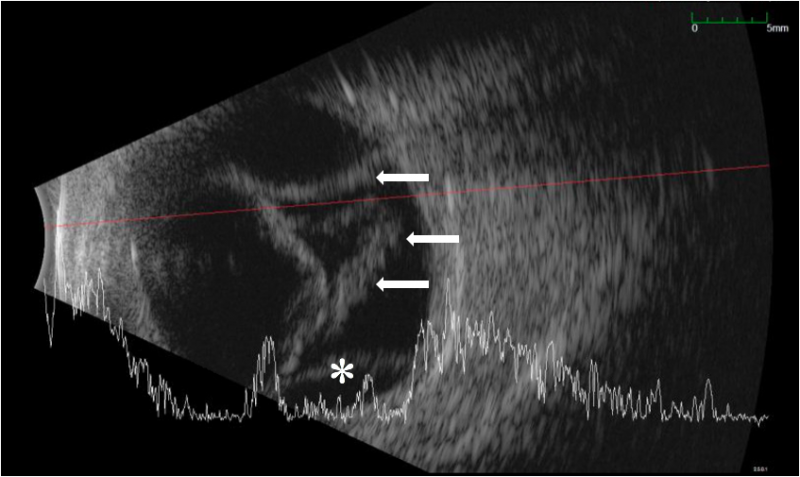
Ultrasound biomicroscopy (UBM) demonstrated a posterior bowing of the iris and diffusely deepened anterior chamber.
Fundus examination demonstrated a rhegmatogenous retinal detachment and choroidal detachment in the right eye and a normal fundus appearance in the left eye. The constellation of findings was consistent with Iris Retraction Syndrome (IRS).
Iris Retraction Syndrome (IRS) DISEASE entity
Iris retraction syndrome (IRS) is a rare condition that is characterized by a backbowing of the peripheral iris with an apposition of the iris body to the anterior surface of the lens.
This results in a substantial deepening of the anterior chamber in a manner that is opposite in configuration to the iris bombe. IRS is typically seen in the setting of a retinal detachment and hypotony.
The most significant risk factor for the Iris retraction syndrome (IRS) is the presence of an underlying retinal detachment. Chronic ocular inflammation, a secluded pupil, and hypotony are also associated with this condition.
IRS has also been reported postoperatively; one instance occurred six months after cataract extraction and posterior chamber intraocular lens (IOL) implantation with pupillary block, another developed four weeks after pars plana vitrectomy in the setting of a secluded pupil, and a third occurred one week after clear cornea phacoemulsification with sulcus IOL placement.
In all three cases, an underlying rhegmatogenous retinal detachment (RRD) was discovered and repaired with subsequent restoration of normal iris configuration.
Physical examination
Visual acuity is usually poor and may count fingers or worse in the setting of a subacute or chronic retinal detachment.
A pupillary exam generally reveals a minimally reactive pupil as a result of near-complete or complete (360 degrees) posterior iris synechiae with central iris-lens apposition. Although hypotony is usually seen in these cases, the intraocular pressure may also be normal.
Slit lamp examination may reveal a mild to moderate degree of intraocular inflammation characterized by corneal edema (microcystic edema or Descemet’s folds), anterior chamber reaction (cell and flare), and posterior iris synechiae.
The anterior chamber is significantly deepened, and the gonioscopy reveals a wide open angle due to retrodisplacement of the peripheral iris away from the angle.
The iris body is opposed to the anterior lens face with the disappearance of the posterior chamber. Cataract formation may also result as a consequence of aqueous diversion.
Ciliochoroidal detachment or effusions may also be seen especially in the setting of hypotony.
Fundus examination and B-scan ultrasonography typically reveal some combination of retinal detachment, choroidal detachment, or PVR if the condition is longstanding.
Iris retraction syndrome (IRS) Signs and Symptoms
Painless vision loss is the most common presenting symptom in IRS due to RRD. Additionally, signs and symptoms of intraocular inflammation may be present including injection, tearing, and photophobia.
Diagnostic Procedures
Diagnosis is made via slit lamp biomicroscopy, gonioscopy, fundoscopy, and B-scan ultrasonography.
Ultrasound biomicroscopy may also provide greater detail of anterior segment structures in the setting of iris retraction syndrome.
Iris retraction syndrome (IRS) MANAGEMENT
Medical therapy:
Pharmacologic dilation with disruption of the central posterior synechiae has been shown to result in the resolution of iris retraction due to the re-formation of the posterior chamber and anterior displacement of the iris body away from the lens surface.
However, in the case of longstanding or permanent synechiae, medical management is unlikely to provide any benefit.
Surgery:
Surgical options that can be considered include pars plana vitrectomy with iris synechiolysis or scleral buckle with surgical iridectomy.
However, in cases of longstanding RRD or PVR, visual prognosis is inherently poor and repair may be unlikely to provide significant benefit.
In these cases, laser peripheral iridotomy can be considered to relieve the IRS and prevent conversion to iris bombe.
Complications:
Patients with untreated Iris retraction syndrome (IRS) can spontaneously convert to iris bombe configuration with secondary angle closure.
Longstanding inflammation in the setting of IRS with an untreated RRD or PVR will typically lead to a blind, phthisical eye, necessitating enucleation.
Prognosis:
Visual prognosis is dependent on the age of the RRD causing the IRS. The shorter the amount of time between onset of RRD and surgical repair, the more favorable the prognosis. Longstanding RRD with PVR tends to have a very poor prognosis.
HOW TO TAKE SLIT-LAMP EXAM IMAGES WITH A SMARTPHONE?
Smartphone slit-lamp photography is the new advancement in the field of science and technology in which photographs of the desired slit-lamp finding can be taken with smartphones by using the slit-lamp adapters.
Slit-lamp Smartphone photography
REFERENCES
- Campbell DG. Iris retraction associated with rhegmatogenous retinal detachment syndrome and hypotony. A new explanation. Arch Ophthalmol. 1984;102(10):1457-63.
- Greenfield DS, Bellows AR, Asdourian GK, Kachadoorian HA. Iris retraction syndrome after intraocular surgery. Ophthalmology. 1995 Jan;102(1):98-100.
- Morinelli EN, Gentile R, Stegman Z, Liebmann JM, Shabto U, Ritch R. Ultrasound biomicroscopic features of iris retraction syndrome. Ophthalmic Surg Lasers. 1996 Apr;27(4):257-62.
- Geyer O, Neudorfer M, Rothkoff L, Michaeli-Cohen A, Lazar M. Iris retraction syndrome associated with nonrhegmatogenous retinal detachment. Acta Ophthalmol Scand. 1998;76(5):617‐619.
- Kahook M, Raju L, Schuman J, Noecker R. Iris Retraction Syndrome After Clear Cornea Phacoemulsification. The Internet Journal of Ophthalmology and Visual Science. 2004;3(2).

{kind=link}