
DISEASE
Advancing Wavelike Epitheliopathy (AWE) is an uncommon disease characterized by well-demarcated, thickened, coarse plaques forming on the cornea.

These have a wavelike or frond-like appearance on slit lamp exam and typically expand from the superior limbus toward the center of the cornea.
Pathological samples of debrided epithelium show no sign of dysplasia or cellular irregularity, and the conjunctiva is spared.
The cause of Advancing Wavelike Epitheliopathy (AWE) is currently poorly understood. Most theories postulate that AWE is a response to irritation to the corneal epithelial stem cells.
Previous ocular surgeries, topical medications, contact lenses, chemical exposure, or inflammatory disorders have been identified as possible stimuli.
Medications that have been implicated in causing AWE include 5-fluorouracil, mitomycin C and interferon, topical antiglaucoma medications, contact lens solution and contact lens wear, and acyclovir.
Illnesses that have been associated with AWE include atopic dermatitis, acne rosacea, and ocular cicatricial pemphigoid. Surgery, toxic chemical exposure, infection, and ocular trauma are also risk factors for the disease.
Diagnosis
Advancing Wavelike Epitheliopathy (AWE) is diagnosed clinically with confocal microscopy and slit lamp exam. Additionally, tissue obtained during treatment should be sent for cytological analysis to confirm the diagnosis of AWE.
Physical examination
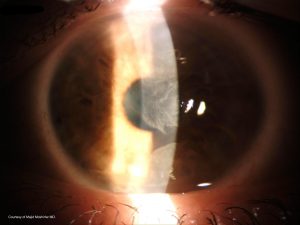
Wavelike plaques with well-defined borders are present, arising from the superior limbus and spreading toward the central cornea.
A granular texture with sclerotic scatter is visible on the corneal surface, and a subepithelial haze is sometimes appreciable.
No infiltrates or discrete inclusions are found. Fluorescein reveals a punctate staining pattern, also with distinct margins as visible with the slit lamp.
Atypical, elongated cells may be seen on confocal microscopy. These have a large nuclear-cytoplasmic ratio, loss of visible cellular borders, and hyperreflective nuclei.
Symptoms
Patients present with chronic or progressive blurry vision, occasionally with periods of remission, over the course of months to years.
Ocular irritation, redness, and foreign body sensation are the most common presenting symptoms. Rarely, patients may be asymptomatic with small lesions that do not obstruct the visual axis. In these patients, simply removing causative agents may be sufficient for complete resolution.
MANAGEMENT
Empiric silver nitrate solution applied topically after corneal epithelial debridement is the established treatment for Advancing Wavelike Epitheliopathy (AWE). Other therapies have been used or proposed as described below.
Medical therapy
Cyclosporine, topical retinoids, interferon alpha-2b, and autologous topical serum drops are all theoretical treatments for AWE as these have been proven effective in other partial limbal stem cell deficiencies (LSCDs).
These have not been formally reported in AWE but may be useful given the similarities between AWE and other LSCDs.
Further clinical trials are necessary to prove this theory. Recently, a case report demonstrated improvement after the use of 5-FU and preservative-free tears.
Topical steroids and artificial tears have been used and rarely provided improvement of AWE symptoms. The use of antibiotics, hypertonic saline, and bandage contact lenses also demonstrate no improvement in symptoms.
Medical follow up
If medical therapy alone is attempted for the treatment of Advancing Wavelike Epitheliopathy (AWE), the patient should be followed closely to observe and prevent the progression of the disease.
Surgery
Identification and elimination of abnormal epithelium are important. As a temporizing measure, corneal epithelial debridement may be performed.

Topical steroids and artificial tears may be used initially. Removal of diseased tissue results in temporary improvement of symptoms, but epitheliopathy often recurs within months.
Standard therapy for Advancing Wavelike Epitheliopathy (AWE) is comprised of corneal epithelial debridement with the empiric application of topical 1% silver nitrate solution.
This is applied to the superior limbus, as described below. It is suggested that the silver nitrate chemically alters the abnormal limbal stem cells responsible for the disease, allowing them to regain normal functioning.
Another theory suggests that silver nitrate or liquid nitrogen causes apoptosis of the abnormal cells, allowing normal stem cells to repopulate the corneal surface with healthy epithelium.
Symptoms typically resolve within two weeks of silver nitrate treatment. The irregular tissue is replaced with normal-appearing epithelium, and most patients see a complete return of baseline vision.
Occasionally patients may experience some minor residual vision loss. Liquid nitrogen cryotherapy has also been used with similar efficacy.
Surgical follow-up
The treated eye should be followed closely for signs of infection after treatment, with a follow-up appointment within two weeks of treatment. Bandage contact lenses may be removed after 3-4 days.
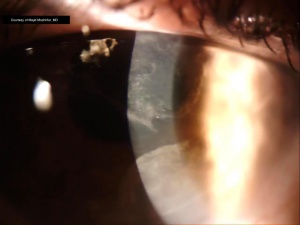
HOW TO TAKE SLIT-LAMP EXAM IMAGES WITH A SMARTPHONE?
Smartphone slit-lamp photography is the new advancement in the field of science and technology in which photographs of the desired slit-lamp finding can be taken with smartphones by using the slit-lamp adapters.
Slit-lamp Smartphone photography
REFERENCES
- D’Aversa G, Luchs JL, Fox MJ, Rosenbaum PS, Udell IJ. Advancing wave-like epitheliopathy: Clinical features and treatment. Ophthalmology. 1997;104(6):962-969. doi:10.1016/S0161-6420(97)30199-7
- Huang YH, Chu HS, Hu FR, Wang IJ, Hou YC, Chen WL. Recurrent advancing wavelike epitheliopathy from the opposite side of the initial presentation. Cornea. 2008;27(1):111-113.
- Fraunfelder FW. Liquid nitrogen cryotherapy of advancing wavelike epitheliopathy. Cornea. 2006;25(2):196-198. doi:10.1097/01.ico.0000170691.67584.ec
- Gupta S, Selvan H, Markan A, Gupta V. Holi colors and chemical contact keratitis. 2018. doi:10.1038/eye.2017.223
- Babu K, Narasimha Murthy KYK, Ramachandra Murthy K. Wavelike epitheliopathy after phacoemulsification: Role of in vivo confocal microscopy. Cornea. 2007;26(6):747-748. doi:10.1097/ICO.0b013e31804f59f3.
- Caroline PJ, Andre M. Contact Lens Spectrum – Epitheliopathy in Contact Lens Wearers. Contact Lens Spectrum.

{kind=link}