
Idiopathic retinal vasculitis, aneurysms, and neuroretinitis (IRVAN) syndrome typically affects young, healthy individuals.

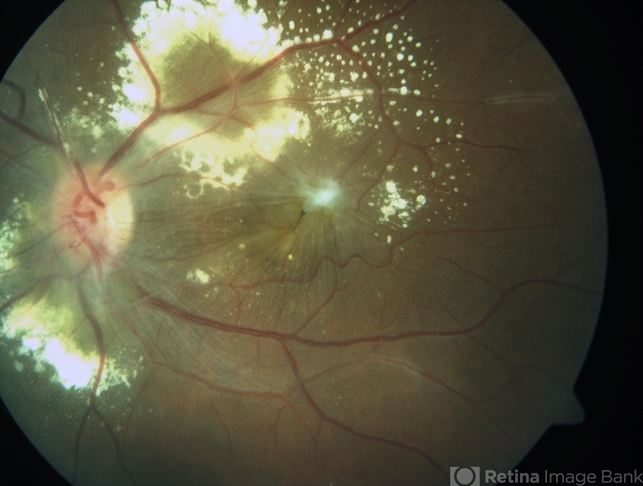
Despite the dramatic fundus appearance seen in this syndrome, these patients are usually asymptomatic. The syndrome includes peculiar vascular abnormalities in the form of multiple aneurysmal dilatations seen along retinal arterioles and optic nerve-head arterioles, which are best appreciated on fluorescein angiography.
Neuroretinitis and retinal vasculitis are seen in all patients, and manifested by staining of the optic nerve head and diffuse leakage from vessels, mainly arterioles, on fluorescein angiography.
The devastating vision-threatening outcomes of this syndrome include exudative retinopathy and extensive peripheral retinal nonperfusion areas, which can eventually lead to neovascularization. This review summarizes current knowledge on diagnostic and treatment strategies.
Diagnostic procedures
Fluorescein angiography:
Fluorescein angiography highlights arteriolar abnormalities. The aneurysms are more evident and the alterations in arteriolar caliber are more obvious.
Leakage of fluorescein from the aneurysms is apparent. Patients with IRVAN usually have optic nerve head staining. Of course, disc and/or retinal neovascularization shows marked fluorescein leakage.
The areas of peripheral non-perfusion are easier to appreciate with fluorescein angiography, especially wide-field fluorescein angiography.
Indocyanine green angiography:
The aneurysmal dilatations showed uniform staining. No abnormalities were seen in the choroidal vessels; in particular, no aneurysms of the choroidal vessels have been observed.
For example, the retinal abnormalities and macroaneurysms in IRVAN are more clearly imaged with ICG angiography, especially at the very late stages, but the leakage, ischemia, and retinal neovascularization are still best delineated with FA.

Optical coherence tomography:
It is useful to assess macular edema, vitreoretinal traction over both the macula and optic nerve head, neovascular tufts in the posterior pole and epiretinal membrane, as an example:
Optical coherence tomography angiography ( OCT-A ):
OCT-A is a dye-free, noncontact modality to image the eye. It is a noninvasive imaging modality that provides three-dimensional images of the retina and choroidal microvasculature in vivo.
OCT-A has its clinical shortcomings and is less useful for identification of retinal vasculitis
- It doesn’t show leakage
- Patients with poor fixation are difficult to image effectively.
- Opaque media such as vitreous hemorrhage blocks the OCT signal and decreases the quality of the angiography.
- Although widefield OCT-A will allow for imaging of the vascular layers, likely out to the mid-periphery and vortex veins, ultra-widefield FA will still provide information about retinal capillary perfusion out to the ora serrata.
Differential diagnosis
At presentation, the physician must distinguish clinical elements of this interesting disease: arterial macroaneurysms, lipid exudation, retinal periphery capillary dropouts, and neovascularization.
The syndrome’s striking ophthalmoscopic picture is not shared by any other disease. However, four principal conditions may be diagnosed initially.
The first is idiopathic retinal vasculitis if the aneurysmal dilations are not noticed. Careful ophthalmoscopic and fluorescein angiographic examination should reveal any aneurysmal dilations, if present.
The second is the senile retinal arterial macroaneurysm. This acquired macroaneurysm is usually found in older patients with a history of high blood pressure and/or cardiovascular diseases. It usually is single, mostly unilateral, located temporal to the optic nerve along the midsegment of an artery, and associated with hemorrhage.
Although there may be capillary telangiectasis surrounding the macroaneurysm, there is no peripheral nonperfusion or signs of inflammation.
Patients with IRVAN are otherwise healthy young people and arterial macroaneurysms are bilateral and multiple. The third element in the differential diagnosis is Coats´ disease.
Patients with Coats’ disease have a unilateral presentation with no signs of intraocular inflammation. The aneurysms of Coats’ disease usually involve more than one element of the vascular circuit and may involve the arteries, capillaries, and veins.
The aneurysms in Coats’ disease do not involve arterial bifurcations and they are observed in the mid and far periphery usually surrounded by abundant circinate lipid exudation.
Finally, peripheral telangiectasias are irregular in shape compared to aneurysms. The fourth condition is Eales´ disease.
Peripheral retina non-perfusion is almost always present with retinal neovascularization and sometimes arising from the optic disc.
Nevertheless, it is not possible to observe typical fusiform or “tied-knot ” arterial aneurysms from IRVAN syndrome.
Management
Currently, retinal laser photocoagulation and the use of intravitreal injections of anti-vascular endothelial growth factor antibodies (anti-VEGF ) are considered within the first line of treatment.
Interestingly, arterial macroaneurysms may regress or vanish after treatment or during follow-up.

General treatment
- Observation: Basha et al have published a pediatric case with IRVAN, with one eye treated and the other eye untreated. A long-term follow-up demonstrated that observation is a consideration in IRVAN syndrome if the vision remains good with hard exudation.
Medical therapy
Corticosteroids:
Patients affected with IRVAN have been treated with corticosteroids in an attempt to reduce any inflammatory worsening of their ophthalmoscopic appearance.
Unfortunately, corticosteroids have not been particularly useful. Although corticosteroids undoubtedly decrease inflammation, much of the morbidity of IRVAN results from chronic secondary changes such as persistent leakage from the aneurysms and vitreous hemorrhage from the neovascularization.
- Systemic use: Prednisone 1mg/kg daily or intravenous
- Intravitreal injections: Triamcinolone Acetate and Dexamethasone implant to treat chronic macular edema.
Anti-VEGF intravitreal injections:
Pegaptanib ( MACUGEN ), Bevacizumab ( AVASTIN ), Ranibizumab ( LUCENTIS ) , and Aflibercept ( EYLEA ) have been used for treating IRVAN syndrome in patients with macular edema, retinal ischemia and neovascularization of the eye.
Immunosuppressive drugs:
Cheema et al and Samalia et al showed improvement in two patients treated with infliximab, an anti-TNF. TNFα might be a causative factor in mediating inflammation and causing tissue destruction in IRVAN patients.
Saatchi et al used oral azathioprine as an adjuvant in a patient with IRVAN. Ameratunga et al used monthly cycles of pulsed intravenous methylprednisolone 1 gm on 3 consecutive days for 7 months along with mycophenolate mofetil and oral prednisone 10 mg daily.
Medical follow up
Follow-up depends on the clinical condition. IRVAN patients should be followed at least every 3 months until stabilization.
Surgery
Thermal Focal Laser and Peripheral Retinal Photocoagulation:
Focal laser treatment to the macroaneurysms may decrease the amount of lipid exudation but carries the risk of causing focal occlusion of the retinal arteriole, thus its use is controversial.
Laser spots may be applied surrounding macroaneurysm areas but never directly. Laser-induced arteriolar occlusion has caused some patients to lose substantial visual acuity.
Panretinal photocoagulation to the peripheral areas of nonperfusion is performed in patients even before retinal/optic disc neovascularization appears.

Several laser sessions may be required for each eye. The aim of this treatment is to cause a regression of the new vessels. Some patients with substantial amounts of vitreous hemorrhage have required vitrectomy and laser endo photocoagulation to treat bleeding areas of retinal neovascularization.
Although retinal and vitreous hemorrhages occur from typical senile retinal arterial macroaneurysms, bleeding from the aneurysmal dilations of IRVAN is not common.
Peripheral cryotherapy:
Some authors have used this procedure, especially when opaque media is present and peripheral laser treatment cannot be applied.
Pars Plana Vitrectomy
Indications:
- Vitreous Hemorrhage that persists for more than 1-2 months.
- Dense vitreous hemorrhage (intravitreal blood/clots do not allow to see optic nerve head and/or retina details.
- Severe loss of vision secondary to vitreous hemorrhage which does not allow for treating a patient.
- Tractional retinal detachment, due to proliferative retinopathy, especially if the center of the retina (macula ) is off. Severe cases may need lensectomy, core vitrectomy, separation of posterior hyaloid, peeling of epiretinal membranes and vitreous base for eliminating vitreoretinal traction, and silicone oil for a long-term vitreous tamponade.
Would you have interest in taking retinal images with your smartphone?
Fundus photography is superior to fundus analysis as it enables intraocular pathologies to be photo-captured and encrypted information to be shared with colleagues and patients.
Recent technologies allow smartphone-based attachments and integrated lens adaptors to transform the smartphone into a portable fundus camera and Retinal imaging by smartphone.
RETINAL IMAGING BY YOUR SMARTPHONE
References
- Basha M, Brown GC, Palombaro G, Shields CL, Shields JA. Management of IRVAN syndrome with observation. Ophthalmic Surg Lasers Imaging Retina. 2014 May 1;45.
- Krishnan R, Shah P, Thomas D. Subacute idiopathic vasculitis, aneurysms and neuroretinitis (IRVAN) in a child and review of paediatric cases of IRVAN revealing preserved capillary perfusion as a more common feature. Eye (Lond). 2015;29:145–151.
- DiLoreto DA Jr, Sadda SR. Idiopathic retinal vasculitis, aneurysms, and neuroretinitis (IRVAN) with preserved perfusion. Retina. 2003;23:554–557.
- Ishikawa F, Ohguro H, Sato S, Sato M, Yamazaki H, Nakazawa M.A case of idiopathic retinal vasculitis, aneurysm, and neuroretinitis effectively treated by steroid pulse therapy. Jpn J Ophthalmol. 2006 Mar-Apr;50(2):181-5.
- Empeslidis T, Banerjee S, Vardarinos A, Konstas AG. Dexamethasone intravitreal implant for idiopathic retinal vasculitis, aneurysms, and neuroretinitis. Eur J Ophthalmol. 2013;23:757–760.
- Mitry D, Schmoll C, Hegde V, Borooah S, Singh J, Bennett H.Use of pegaptanib in the treatment of vitreous haemorrhage in idiopathic retinal vasculitis. Eye (Lond). 2008 Nov;22(11):1449-50.

{kind=link}