
DISEASE
Incontinentia pigmenti (IP), also known as Bloch-Sulzberger syndrome, is a rare X-linked dominantly inherited syndrome manifesting at birth or early childhood.


The cardinal feature is the appearance of characteristic progressive skin lesions, first presenting as vesiculobullous lesions and then progressing to whorl-like pigmentary lesions over four stages.
IP also includes eye abnormalities, mostly occurring in the retina. The retinal findings stem from vascular occlusion and include neovascularization, hemorrhages, absence of the foveal pit, and exudative and tractional retinal detachments.
Pathologic changes in the central nervous system, teeth, and hair are also common in Incontinentia pigmenti (IP). Diagnosis is based on clinical systemic and ocular exams, as well as genetic testing.
There is no treatment for the disease as a whole; however, symptoms may be managed by medical or surgical intervention.
Ophthalmologic Exam and Findings
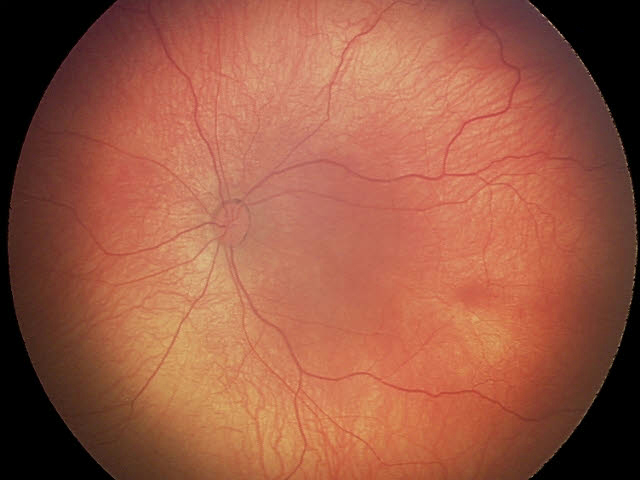
A thorough eye exam must be performed on those suspected of IP. Eye findings are seen in 35-40% of those with IP.
Both retinal and non-retinal findings are seen in Incontinentia pigmenti (IP). Retinal findings are common and include avascularity, neovascularization, hemorrhages, absence of a foveal pit, optic nerve atrophy, and exudative and retinal tractional detachments.
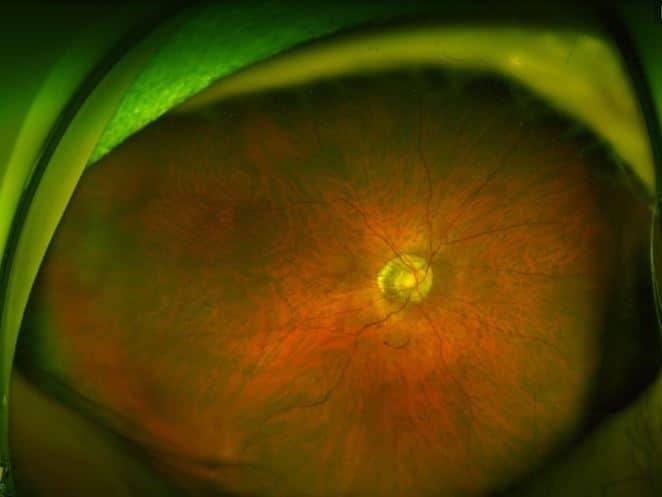
Retinal detachment is the most commonly diagnosed eye finding in IP. Due to the vaso-occlusive nature of IP, a cherry red foveal spot may be seen as choroidal perfusion and is not typically affected; however, observing the occlusive event in its acute stage is rare.
A blunted foveal pit and absence of normal parafoveal vascular pattern are also characteristic of IP, caused by vessel occlusion and subsequent vascular remodeling.
Occlusions of retinal vessels in the macula and the periphery are typically seen and are often accompanied by diffuse mottled hypopigmentation.
Retinal detachments, if present, nearly always occur within six years of age and are relatively rare in older patients. Additional non-retinal ocular manifestations include cataracts, uveitis, strabismus (18%), conjunctival pigmentation, optic atrophy (5%), and nystagmus. Phthisis bulbi can be the result of ocular Incontinentia pigmenti (IP).
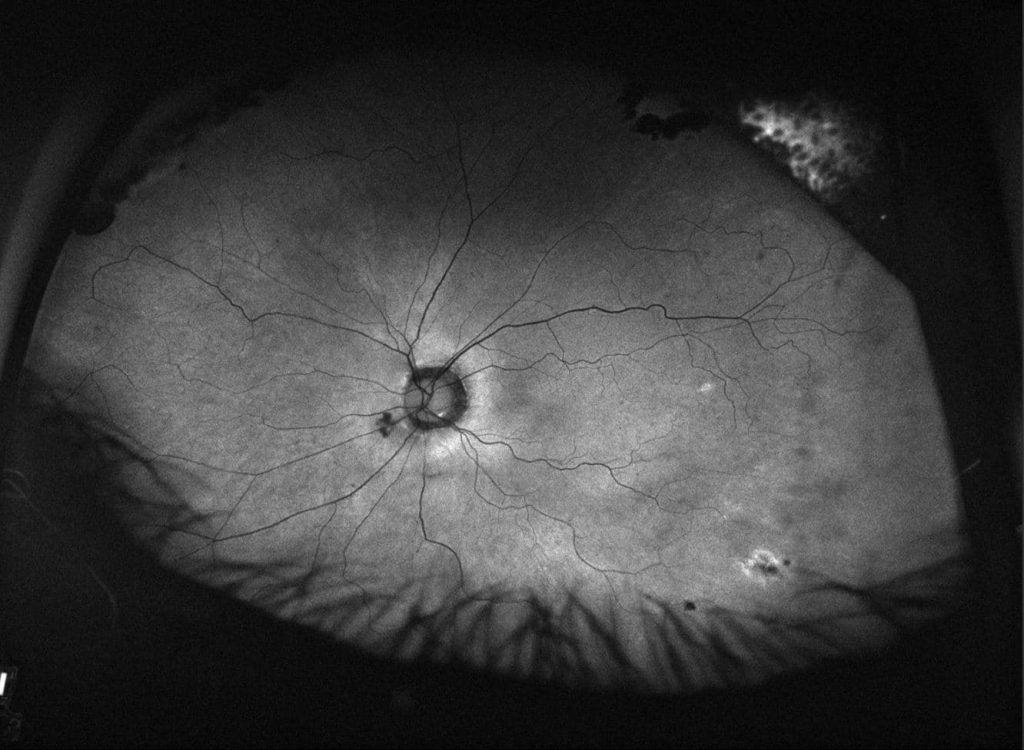
An avascular peripheral retina is a significant feature of IP’s retinal manifestations. Typically, the neovascularization of the retina is more pronounced in the periphery, similar to retinopathy of prematurity.
Tufts of neovascularization can be found at the edges of the avascular retina. Fluorescein angiography is a critical study in the ophthalmic investigations for IP.
Often, enlargement of the foveal avascular zone is seen, which can be accompanied by large areas of avascularity anywhere in the retina.
Cortical blindness may sometimes be present due to vascular occlusions in the occipital cortex in IP. Neurologic consultation and MRI brain imaging should be obtained to investigate this possibility.
Differential diagnosis
The differential diagnosis for the retinal manifestations of Incontinentia pigmenti (IP) include retinopathy of prematurity, familial exudative vitreoretinopathy, Eales retinopathy, sickle cell retinopathy, and the Norrie disease spectrum. However, skin findings are not associated with these conditions.
The differential diagnosis for the dermatologic findings in Incontinentia pigmenti (IP) is large and can be divided based on the stage of the skin lesions.
They include congenital herpetic infection, impetigo/epidermolysis bullosa, warts or molluscum contagiosum, hypomelanosis of Ito, scaring, and vitiligo.
Naegeli syndrome is a rare condition affecting the skin and ectoderm which can appear similar to the skin lesions of IP. It does not have significant eye findings.
Management
As IP has a genetic basis, there is no cure and treatment is limited to treating symptoms at this time.
General treatment
Because Incontinentia pigmenti (IP) is a multi-faceted condition, dermatologic, genetic, ophthalmic, neurologic, and dental consultations should be obtained.
Generally, brain imaging should be obtained (MRI) to investigate the occlusive consequences of IP in the brain. EEG should be obtained if seizures are present.
Developmental therapy may be needed. Skin lesions should be managed symptomatically to avoid infection or excessive scarring. Genetic therapies are not currently available for IP.
Ophthalmic treatment
The avascular retina should be treated similarly to retinopathy of prematurity with laser photocoagulation (or cryotherapy) of the avascular retina.
The occurrence of retinal detachments should be monitored with regular ophthalmological exams and surgical repair of detachments should be attempted by a vitreoretinal surgeon if appropriate. Vitrectomy with or without a scleral buckle is commonly performed.
Intravitreal anti-vascular endothelial growth factor has been investigated. While this may be a promising treatment, it has not become the standard of care.
Would you have interest in taking retinal images with your smartphone?
Fundus photography is superior to fundus analysis as it enables intraocular pathologies to be photo-captured and encrypted information to be shared with colleagues and patients.
Recent technologies allow smartphone-based attachments and integrated lens adaptors to transform the smartphone into a portable fundus camera and Retinal imaging by smartphone.
RETINAL IMAGING BY YOUR SMARTPHONE
REFERENCES
- Buinauskiene J, Buinauskaite E, Valiukeviciene S. Incontinentia pigmenti (bloch-sulzberger syndrome) in neonates. Medicina (Kaunas). 2005;41(6):496-9.
- Goldberg MF, Custis PH. Retinal and other manifestations of incontinentia pigmenti (bloch-sulzberger syndrome). Ophthalmology. 1993 Nov;100(11):1645-54.
- Scheuerle A, Ursini MV. Incontinentia pigmenti. In: Pagon RA, Bird TD, Dolan CR, Stephens K, editors. GeneReviews. Seattle (WA): University of Washington, Seattle. All rights reserved; 1993.
- Nelson DL. NEMO, NFkappaB signaling, and incontinentia pigmenti. Curr Opin Genet Dev. 2006 Jun;16(3):282-8.
- Fusco F, Pescatore A, Bal E, Ghoul A, Paciolla M, Lioi MB, et al. Alterations of the IKBKG locus and diseases: An update and a report of 13 novel mutations. Hum Mutat. 2008 May;29(5):595-604.
- Meffert MK, Chang JM, Wiltgen BJ, Fanselow MS, Baltimore D. NF-kappa B functions in synaptic signaling and behavior. Nat Neurosci. 2003 Oct;6(10):1072-8.

{kind=link}