
CASE REPORT
A 51-year-old woman presented with blurred vision in her left eye (LE) for one week. The patient underwent cataract surgery with phacoemulsification and IOL implantation in the capsular bag two months before.

A Zeiss CT ASPHINA 404 [aspheric Hydrophilic acrylic (25%) IOL with hydrophobic surface, Carl Zeiss Meditec Inc., Germany] IOL (-06 diopters) for emmetropia was successfully implanted in the capsule with 360° overlapping of capsular edge onto the anterior IOL optic surface.
All surgical procedures were uneventful. The same IOL was implanted about two months earlier in the RE. Furthermore, the two eyes were known to be affected by high myopia (axial length of 31.15 mm in the RE and axial length of 31.28 mm in the LE) and pseudoexfoliation syndrome (PEX) only in the LE. Her medical history was otherwise unremarkable.
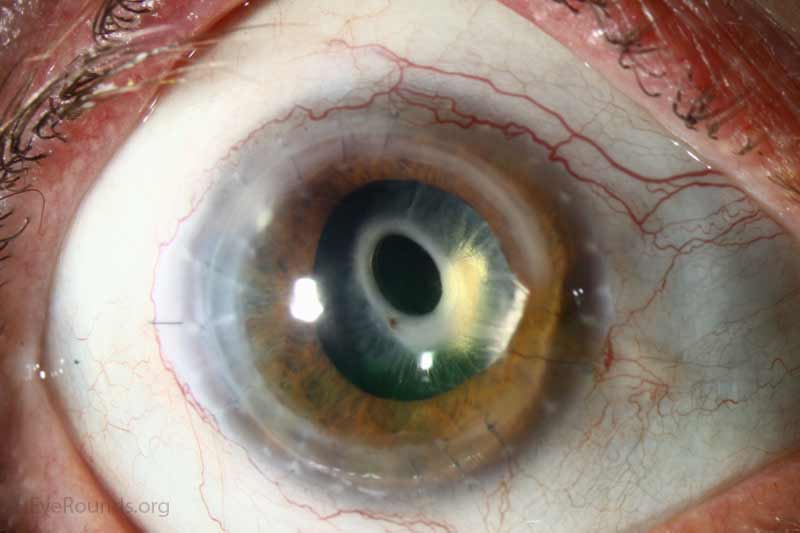
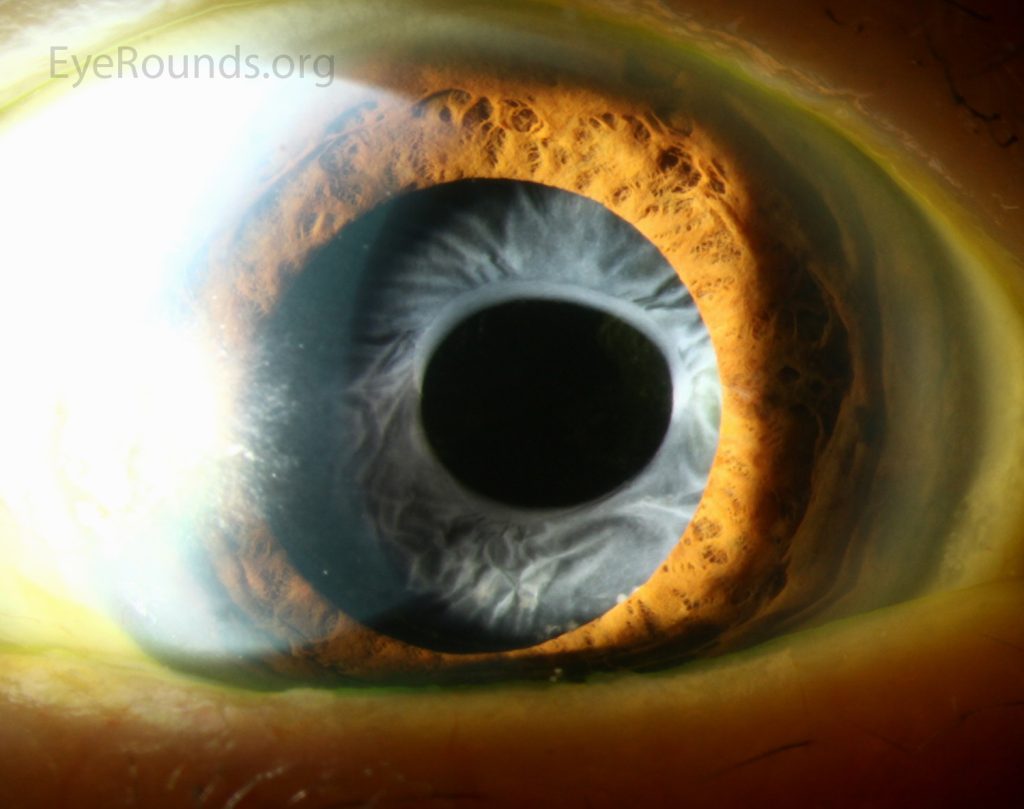
At presentation, the best-corrected visual acuity (BCVA) was 0.0 and 1.0 logMAR in her RE and LE, respectively. Slit lamp anterior segment examination of the LE revealed anterior capsule fibrosis occluding the visual axis. The patient also underwent anterior segment optical coherence tomography (AS-OCT), which revealed the presence of a hyperreflective and thick band adherent to the anterior surface of the IOL.
Because of the insufficient clear media to allow ophthalmoscopy, B-scan ultrasound was performed and no alterations of the retina and vitreous were discerned. A diagnosis of Anterior Capsular Contraction Syndrome was thus made.
Anterior Capsular Contraction Syndrome DISEASE entity
Anterior capsule contraction syndrome commonly described as, Anterior capsule fibrosis and phimosis, is the centripetal constriction and fibrosis of the capsulorhexis following cataract removal.
This is a painless condition that remains asymptomatic unless the constriction progresses into the visual axis potentially resulting in decreased visual acuity, pseudophacodonesis, and occasionally intraocular lens dislocation.
Treatment consists primarily of Nd: YAG relaxing of the anterior capsulotomy of encroaching tissue and recurrence is rare. While the pathogenesis of Anterior Capsular Contraction Syndrome is unknown, a possible cause involves populations of residual viable metaplastic lens epithelial cells (LECs) in or on the capsular bag present after cataract surgery that can undergo mesenchymal transition and differentiation to fiber-like cells.
Metaplasia and fibrosis of these cells contribute to the purse-string contracture and constriction or even complete closure of the anterior capsulotomy. This response may be exaggerated when there is an imbalance between centrifugal and centripetal forces that act on the zonules and the capsulorhexis perimeter.

Anterior Capsular Contraction Syndrome MANAGEMENT
General treatment
Most ophthalmologists perform Nd: YAG LASER anterior capsulotomy which is a simple and painless outpatient procedure. Typically 4 or more approximately 1mm radial nicks placed onto the fibrotic anterior capsular annulus are effective in stopping the progression of contraction of the anterior capsule.
The LASER is set to anterior focus and an energy of 1 to 3mJ. Radial Nicks are preferred, with care taken not to hit the IOL. Some surgeons have tried cutting out an annulus of the capsule using the LASER, but it is not recommended as it deposits in the angle and often leads to raised intraocular pressure.

It is recommended that this be accomplished when phimosis has progressed to less than 4mm to prevent potential late zonular dehiscence.
Surgery
In less severe phimosis without invasion of the optical zone, the first choice of treatment is neodymium: YAG (Nd: YAG) laser capsulotomy while manually peeling the fibrotic membrane is the technique of choice in severe cases with dense fibrous plaques to prevent incomplete reabsorption of loose capsular debris and to decrease the risk of inflammation and recurrence.
HOW TO TAKE SLIT-LAMP EXAM IMAGES WITH A SMARTPHONE?
Smartphone slit-lamp photography is the new advancement in the field of science and technology in which photographs of the desired slit-lamp finding can be taken with smartphones by using the slit-lamp adapters.
Slit-lamp Smartphone photography
REFERENCES
- Joo, C.-K., Shin, J.-A. & Kim, J.-H. Capsular opening contraction after continuous curvilinear capsulorhexis and intraocular lens implantation. J. Cataract Refract. Surg. 22, 585–590 (1996).
- Marcantonio, J. M., Rakic, J. M., Vrensen, G. F. & Duncan, G. Lens cell populations studied in human donor capsular bags with implanted intraocular lenses. Invest. Ophthalmol. Vis. Sci. 41, 1130–41 (2000).
- Davison, J. A. Capsule contraction syndrome. J. Cataract Refract. Surg. 19, 582–9 (1993).
- Lüke, C., Dietlein, T. S., Jacobi, P. C., Konen, W. & Krieglstein, G. K. Massive anterior capsule shrinkage after plate-haptic silicone lens implantation in uveitis. J. Cataract Refract. Surg. 27, 333–6 (2001).
- Hayashi, H., Hayashi, K., Nakao, F. & Hayashi, F. Area reduction in the anterior capsule opening in eyes of diabetes mellitus patients. J. Cataract Refract. Surg. 24, 1105–1110 (1998).
- Hayashi, K., Hayashi, H., Matsuo, K., Nakao, F. & Hayashi, F. Anterior capsule contraction and intraocular lens dislocation after implant surgery in eyes with retinitis pigmentosa. Ophthalmology 105, 1239–43 (1998).

{kind=link}