
DISEASE
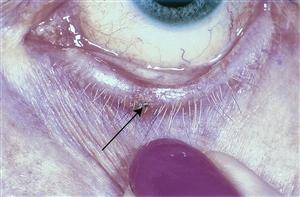
Actinic keratosis is a premalignant squamous lesion. It may appear clinically as erythematous, scaly macules or papules. Lesions are typically present in middle-aged or elderly patients.


Sun-exposed areas are most commonly affected. Squamous cell carcinoma may develop from preexisting actinic keratoses.
Thus, a biopsy of suspected lesions and long-term follow-up is necessary for patients with this condition. The risk of subsequent metastatic dissemination is very low (0.5-3.0%).
The most likely factor that leads to the development of actinic keratosis is sunlight exposure, specifically UVA and UVB sunlight.
Exposure to these forms of radiation leads to a complex series of genetic events which eventually lead to the development of actinic keratosis and squamous cell carcinoma. History of chronic sunlight exposure. Lack of sunscreen use when outdoors. Fairer skin types (Fitzpatrick types I, II)
Diagnosis
A preliminary diagnosis may be made based on the patient’s history and clinical appearance. Examination of skin can be performed with a slit-lamp, dermatoscope, or with the naked eye.
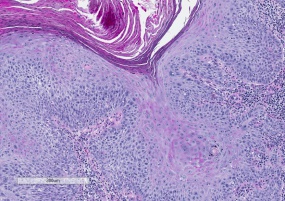
However, a definitive diagnosis of a new lesion requires a biopsy with a review by a pathologist.
- Patients will usually present with a slowly developing scaling and erythematous lesion of the skin.
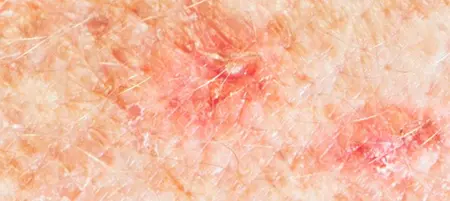
- Erythematous (red), scaly macule (flat pigmented lesion), or papule (solid, elevated lesion) may be present on the skin surface. Multiple lesions may be present.
- The skin of affected areas may feel rough or have a “sandpapery” texture. The lesions may have a round and scaly appearance. Itching or irritation may be present on the skin of affected individuals. It appears clinically as an erythematous, scaly macule or papule.
- Actinic keratoses are most commonly found on the face, lips, ears, back of the hands, forearms, scalp, or neck.
- Lesions with bleeding, persistent itching, growth, or changes may be biopsied to confirm the diagnosis.
MANAGEMENT
Observation, medical, or surgical treatment may be recommended depending on individual circumstances.
Progression to squamous cell cancer is generally slow and in elderly patients with multiple comorbidities, for example, observation may be the best choice.
- Medical therapy
- The following topical medications have been FDA approved for the treatment of Actinic Keratosis.
- 5-fluorouracil (5-FU)
- Imiquimod cream
- Ingenol mebutate gel
- Topical diclofenac gel
- A systematic review compared the relative efficacy of 5-fluorouracil 0.5% in salicylic acid 10% (5-FU/SA) vs. ingenol mebutate (IMB) and imiquimod 2.5%/3.75% (IMI) for actinic keratosis on the face, forehead or scalp. The study showed both treatments to be effective for actinic keratosis.
- Cryotherapy is typically carried out in a dermatologist’s office for facial lesions. Periocular lesions should be treated by an oculofacial plastic surgeon.
- Photodynamic therapy (PDT) has been described as a treatment for actinic keratosis.
- Topical application of ALA to a skin lesion and subsequent illumination of the lesion with red light, and has been shown to be an attractive alternative to cryotherapy with improved aesthetic outcomes.
- TCA chemical peels may be useful in patients with diffuse lesions that are challenging to treat one at a time.
- The following topical medications have been FDA approved for the treatment of Actinic Keratosis.
- Surgical therapy
- Lesions may be completely excised if there is a concern for malignancy. However, in most cases, actinic keratosis may be observed clinically for progression.
- Laser treatments may also be an option if there is no concern for malignancy.
HOW TO TAKE SLIT-LAMP EXAM IMAGES WITH A SMARTPHONE?
Smartphone slit-lamp photography is the new advancement in the field of science and technology in which photographs of the desired slit-lamp finding can be taken with smartphones by using the slit-lamp adapters.
Slit-lamp Smartphone photography
REFERENCES
- Ophthalmic Pathology and Intraocular Tumors, Section 4. Basic and Clinical Science Course. San Francisco: American Academy of Ophthalmology; 20011-12.
- Ortonne, J.-P. (2002), From actinic keratosis to squamous cell carcinoma. British Journal of Dermatology, 146: 20–23. doi: 10.1046/j.1365-2133.146.s61.6.x
- Stockfleth, Eggert, Gillian C. Sibbring, and Ivette Alarcon. “New topical treatment options for actinic keratosis: a systematic review.” Acta dermato-venereologica 96.1 (2016): 17-23.
- R.M. Szeimiesa, S. Karrera, S. Radakovic-Fijanb, A. Tanewb, P.G. Calzavara-Pintonc, C. Zanec, A. Sidoroffd, M. Hempele, J. Ulrichf, T. Proebstleg, H. Mefferth, M. Mulderi, D. Salomonj, H.C. Dittmark, J.W. Bauerl, K. Kernlandm, L. Braathenm, Photodynamic therapy using topical methyl 5-aminolevulinate compared with cryotherapy for actinic keratosis: A prospective, randomized study, Journal of the American Academy of Dermatology, Volume 47, Issue 2, August 2002, Pages 258-262, ISSN 0190-9622.

{kind=link}