
DISEASE “Xanthelasma”
Xanthelasma Palpebrarum (XP) is a benign condition involving cutaneous lesions in the periocular region. It presents as a xanthoma found on the medial aspect of the eyelids.


These lesions do not typically present with functional limitations. It occurs more commonly in women (1.2% incidence rate) than in men (0.3% incidence rate) with a peak incidence at the ages of 30-50 years old.
Nearly half of patients with XP have associated lipid disorders. These include Type II hyperlipidemia, Type IV hyperlipidemia, high total cholesterol, high triglycerides, and low levels of high-density lipoprotein (HDL).
However,
despite the strong association of XP with lipid imbalance, 25-70% of patients are normolipidemic on presentation.
Xanthelasma Diagnosis
XP lesions present as soft, yellow papules or plaques filled with cholesterol at the medial canthus of the eyelids. They can appear as multiple, symmetric lesions that more commonly are found on the upper eyelid than the lower one.

Patients will seek professional treatment for xanthelasma due to cosmetic concerns.
Additionally,
these lesions tend to be permanent and can grow in size with time which may be distressing. From a provider standpoint, the diagnosis can be made clinically.
Biopsy:
Reticular dermis infiltration of foamy macrophages with sparing of the epidermis, papillary dermis, and subcutaneous fatty layer.
The inflammatory infiltrates in the superficial reticular dermis will be perivascular and consist of foam cells with lipid-laden cytoplasmic vacuoles.
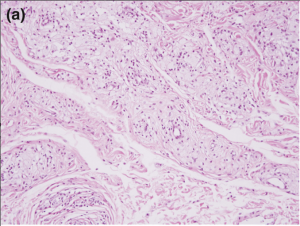
Foam cells, or xanthoma cells, originate from macrophages that have accumulated intracellular cholesterol, lipids, and fat.
MANAGEMENT of Xanthelasma
Conservative therapy begins with a low-fat diet and statins- the therapeutic effect is questionable. Popular treatment options include surgical excision, laser therapy, chemical peel, cryotherapy, and radiofrequency ablation.
Surgical excision of the xanthelasma was one of the earliest treatments, however, post-operative adverse outcomes must be considered.
Risk of cicatricial ectropion, transient hematomas, poor cosmetic outcome, recurrence, and infection are possible.
Trichloroacetic acid (TCA) is commonly used for the peel at a 70% concentration.
Laser therapy utilizes energy to coagulate vessels and damage the perivascular foam cells that make up the lesion.
Cryotherapy causes vasoconstriction and the formation of microthrombi as a result of cell death within XP lesions.
Radiofrequency treatment works by causing electrocoagulation for instant hemostasis and is used in vascular lesions.
REFERENCES
1. Esmat SM, Elramly AZ, Abdel Halim DM, Gawdat HI, Taha HI. Fractional CO2 laser is an effective therapeutic modality for xanthelasma palpebrarum: a randomized clinical trial. Dermatol Surg. Dec 2014;40(12):1349-55. doi:10.1097/DSS.0000000000000172
2. Aggarwal R, Rathore PK. A study evaluating xanthelasma palpebrarum clinically and biochemically. International Journal of Contemporary Medical Research. 2016;3(9):2565-7.
3. Dincer D, Koc E, Erbil AH, Kose O. Effectiveness of low-voltage radiofrequency in the treatment of xanthelasma palpebrarum: a pilot study of 15 cases. Dermatol Surg. Dec 2010;36(12):1973-8. doi:10.1111/j.1524-4725.2010.01770.x
4. Nahas TR, Marques JC, Nicoletti A, Cunha M, Nishiwaki-Dantas MC, Filho JV. Treatment of eyelid xanthelasma with 70% trichloroacetic acid. Ophthalmic Plast Reconstr Surg. Jul-Aug 2009;25(4):280-3. doi:10.1097/IOP.0b013e3181aa9a1f
5. Al Aboud AM, Al Aboud DM. Xanthelasma Palpebrarum. StatPearls. 2021.

{kind=link}