
Case Study
A 29-year-old immunocompetent male presented with blurred vision and floaters in his left eye for one week. He reported mild ocular discomfort and photophobia.


There was no significant systemic history. Best-corrected visual acuity was 20/25 in the affected eye and 20/20 in the fellow eye.
Anterior segment examination revealed mild anterior chamber cells. Fundus examination of the left eye demonstrated focal necrotizing retinitis in the peripheral retina with associated vitritis.
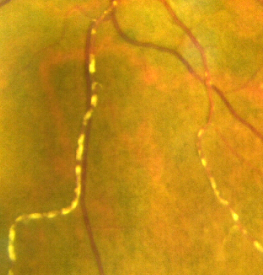
Segmental, discrete, whitish deposits were observed along the retinal arterioles, giving a beaded appearance. The veins were relatively spared.
Fluorescein angiography (FA) showed minimal leakage from the affected arterioles without significant staining of the vessel wall.
Optical coherence tomography (OCT) revealed mild inner retinal hyperreflectivity adjacent to areas of active retinitis.
Polymerase chain reaction (PCR) analysis of aqueous humor confirmed herpes simplex virus infection.
The patient was diagnosed with acute retinal necrosis (ARN) associated with Kyrieleis arteriolitis and was treated with systemic antiviral therapy. The arteriolar plaques gradually resolved with treatment.
Disease Entity
Kyrieleis arteriolitis is a distinctive form of segmental retinal arteriolar inflammation characterized by the presence of focal, white, bead-like deposits along retinal arterioles.
These deposits are classically associated with infectious posterior uveitis, particularly toxoplasmosis and herpetic retinitis, including acute retinal necrosis.
First described by Kyrieleis in 1933, this condition is considered a clinical sign rather than a standalone disease entity. It represents a specific vascular response to intraocular infection or inflammation.
The defining feature is the presence of segmental intra-arteriolar plaques that appear as discrete, refractile white lesions aligned along the course of retinal arterioles, often adjacent to areas of active retinitis.
Pathophysiology
The exact pathogenesis of Kyrieleis arteriolitis remains incompletely understood, but it is believed to involve localized inflammatory deposition within or adjacent to the retinal arteriolar wall.
Proposed mechanisms include:
- Deposition of inflammatory cells or immune complexes within the vessel wall
- Focal endothelial dysfunction
- Perivascular infiltration secondary to adjacent retinal infection
Unlike typical retinal vasculitis, Kyrieleis arteriolitis appears to involve intraluminal or intramural deposition rather than diffuse perivascular inflammation.
Histopathologic correlation is limited, but clinical imaging suggests that the plaques are non-occlusive and do not significantly impair blood flow.
An important distinguishing feature is that these lesions typically do not exhibit significant leakage on fluorescein angiography, indicating relative preservation of vascular integrity.
Epidemiology
Kyrieleis arteriolitis is rare and occurs in association with specific infectious retinal conditions.
It is most commonly reported in:
- Ocular toxoplasmosis
- Acute retinal necrosis (ARN)
- Other herpetic retinitides
The condition can occur in both immunocompetent and immunocompromised individuals, depending on the underlying cause.
There is no clear age, sex, or racial predilection, as the epidemiology reflects that of the associated infectious diseases.
Clinical Features
Symptoms are primarily related to the underlying retinal infection rather than the arteriolitis itself.
Common presenting symptoms include:
- Blurred vision
- Floaters
- Photophobia
- Mild ocular discomfort
The onset is typically subacute.
Visual acuity varies depending on:
- Location of retinitis
- Degree of vitritis
- Macular involvement
Kyrieleis plaques themselves are asymptomatic but serve as an important diagnostic clue.
Examination Findings
Anterior Segment
- Mild anterior chamber inflammation may be present
- Keratic precipitates in some cases
Posterior Segment
Characteristic findings include:
- Segmental, white, bead-like deposits along retinal arterioles
- Sparing of retinal veins
- Adjacent areas of active retinitis
- Vitritis of variable severity
The plaques are typically:
- Discrete and well-defined
- Located along the length of arterioles
- Non-contiguous (segmental distribution)
Fluorescein Angiography (FA)
FA findings are distinctive:
- Minimal or no leakage from affected arterioles
- No significant staining of vessel walls
- Normal or near-normal perfusion
This helps differentiate Kyrieleis arteriolitis from true retinal vasculitis.
Optical Coherence Tomography (OCT)
- Localized inner retinal hyperreflectivity near areas of inflammation
- Possible disruption of retinal layers in necrotizing retinitis
Optical Coherence Tomography Angiography (OCTA)
- Preserved flow in affected arterioles
- No significant capillary dropout attributable to plaques
Differential Diagnosis
Kyrieleis arteriolitis should be differentiated from other forms of retinal vascular inflammation.
Key differential diagnoses include:
- Retinal vasculitis (e.g., Behçet disease, sarcoidosis)
- Frosted branch angiitis
- Embolic phenomena
- Infectious retinal vasculopathy
In retinal vasculitis:
- There is diffuse perivascular sheathing
- FA shows leakage and staining
In embolic disease:
- Lesions are typically located at vascular bifurcations
- Associated with vascular occlusion
The absence of leakage on FA and the characteristic segmental arteriolar plaques are key distinguishing features.
Diagnosis
Diagnosis is clinical and based on recognition of characteristic fundus findings in the context of infectious retinitis.
Key diagnostic elements include:
- Segmental white plaques along retinal arterioles
- Association with active retinal infection
- Minimal leakage on fluorescein angiography
- Sparing of veins
Additional investigations are directed toward identifying the underlying cause:
- PCR testing for viral pathogens
- Serologic testing for toxoplasmosis
- Imaging as indicated
Kyrieleis arteriolitis itself does not require separate diagnostic testing.
Management
Management is directed at the underlying infectious etiology, as Kyrieleis arteriolitis resolves with treatment of the primary condition.
Infectious Causes
- Antiviral therapy (e.g., acyclovir) for herpetic infections
- Anti-toxoplasma therapy (e.g., pyrimethamine, sulfadiazine)
Adjunctive Therapy
- Corticosteroids may be used to control inflammation once antimicrobial therapy is initiated
The arteriolar plaques typically regress gradually with successful treatment.
No specific therapy is required for the vascular lesions themselves.

Prognosis
The prognosis of Kyrieleis arteriolitis depends on the underlying retinal disease.
Key points:
- The arteriolar plaques are generally reversible
- They do not typically cause vascular occlusion
- Visual outcome is determined by the severity and location of retinitis
With appropriate treatment, the plaques often resolve without permanent vascular damage.
However, complications from the primary infection—such as retinal necrosis or scarring—may affect visual prognosis.
Would you have interest in taking retinal images with your smartphone?
Fundus photography is superior to fundus analysis as it enables intraocular pathologies to be photo-captured and encrypted information to be shared with colleagues and patients.
Recent technologies allow smartphone-based attachments and integrated lens adaptors to transform the smartphone into a portable fundus camera and Retinal imaging by smartphone.
RETINAL IMAGING BY YOUR SMARTPHONE
References
- American Academy of Ophthalmology. Basic and Clinical Science Course (BCSC): Uveitis and Ocular Inflammation. San Francisco, CA: AAO; latest edition.
- Yanoff M, Duker JS. Ophthalmology. 5th ed. Elsevier; 2019.
- Kyrieleis W. Über arterielle Gefäßveränderungen bei Chorioretinitis. Klin Monbl Augenheilkd. 1933;91:741–746.
- Cunningham ET Jr, Short GA. Kyrieleis plaques in ocular toxoplasmosis. Ophthalmology. 1998;105(6):1141–1145.
- Coats DK, Paysee EA. Kyrieleis arteriolitis is associated with acute retinal necrosis. Am J Ophthalmol. 2001;131(3):394–396.
- Pichi F, Ciardella AP, Cunningham ET Jr. Imaging of infectious retinal vasculitis. Ophthalmol Retina. 2018;2(6):563–575.
RETINAL IMAGING BY YOUR SMARTPHONE

RETINAL IMAGING BY YOUR SMARTPHONE
{kind=link}