
Case Study
A 34-year-old woman presented with recurrent episodes of transient blurred vision in her right eye over the past two months. Each episode lasted approximately 5–10 minutes and resolved spontaneously without residual deficit.

She described associated shimmering visual disturbances but denied headache, eye pain, or systemic symptoms.
Her medical history was unremarkable, although she reported a tendency toward cold-induced digital color changes suggestive of vasospastic phenomena.
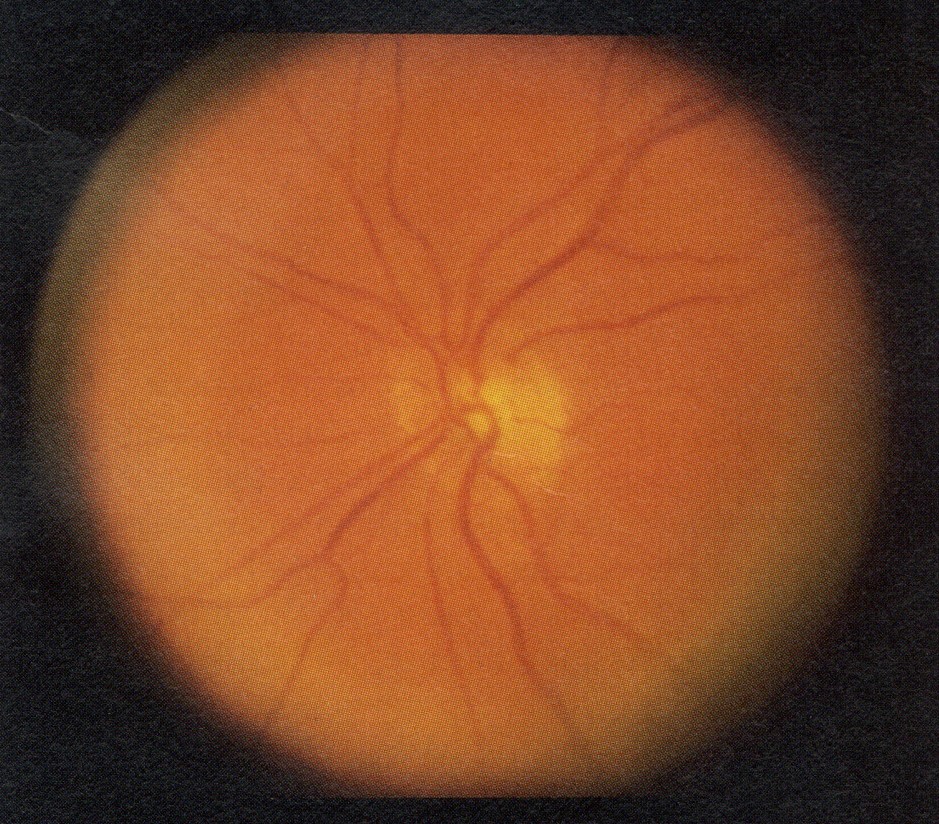
Best-corrected visual acuity was 20/20 in both eyes. Anterior segment examination was normal. Fundus examination between episodes was unremarkable, with no evidence of emboli or vascular occlusion.
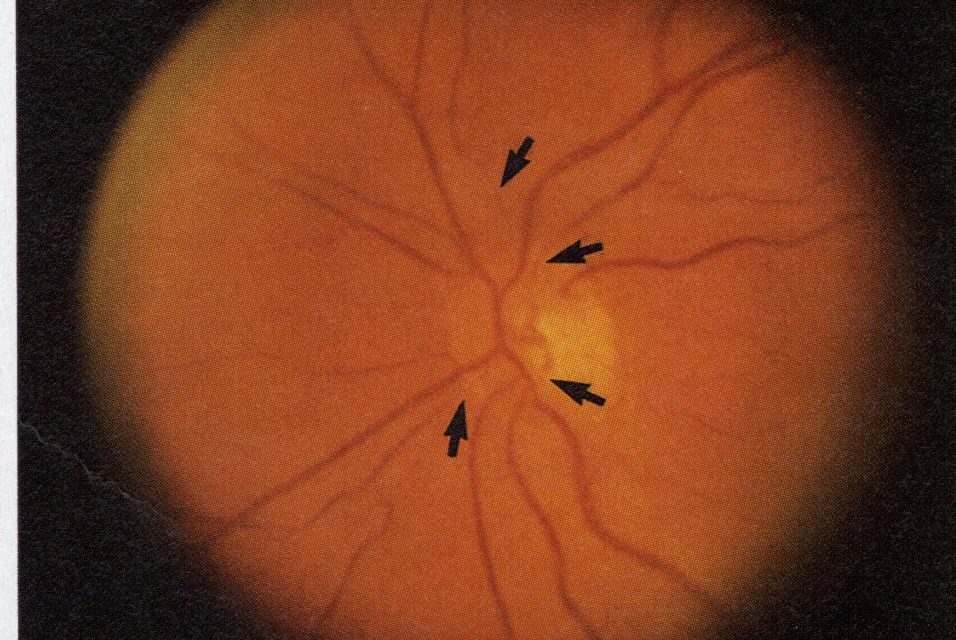
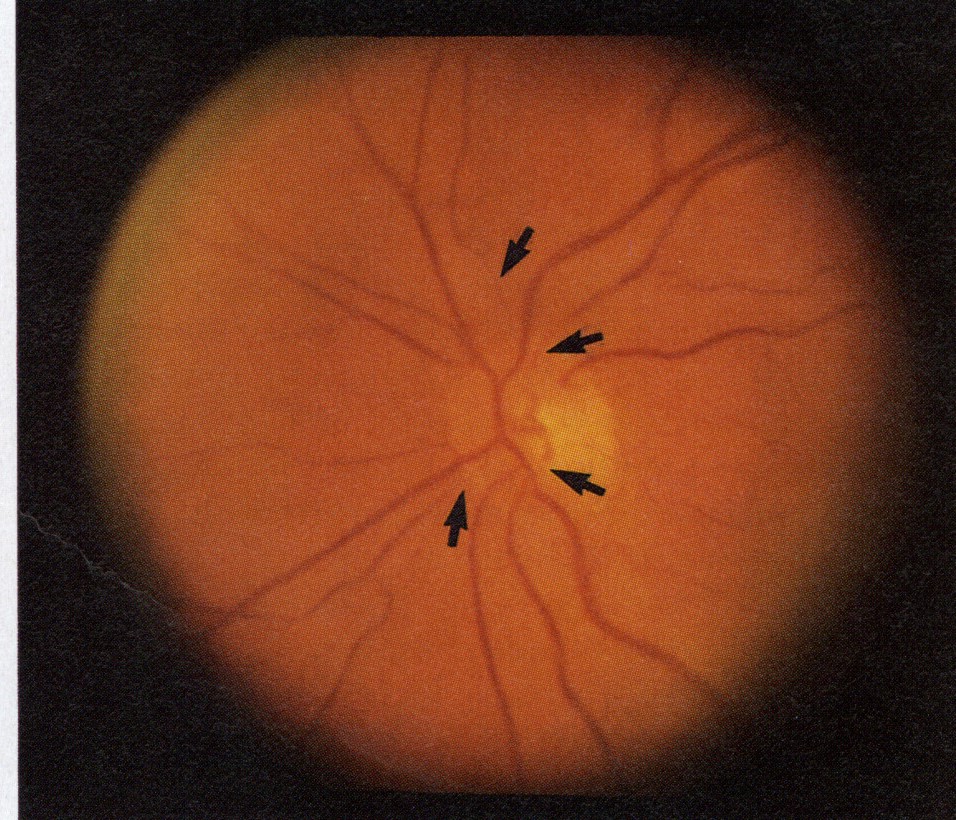
During an observed episode, segmental narrowing of a branch retinal arteriole was noted.
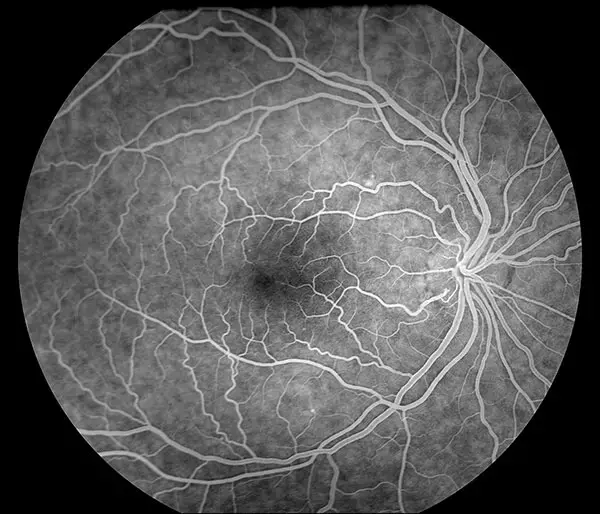
Fluorescein angiography (FA) performed shortly after symptom onset demonstrated delayed filling of the affected arteriole without evidence of embolus or leakage.
Optical coherence tomography (OCT) was normal. Systemic evaluation, including cardiovascular and neurologic workup, was unremarkable.
A diagnosis of idiopathic retinal vasospasm was made. The patient was managed conservatively with lifestyle modification and a trial of calcium channel blockers, resulting in a reduction in episode frequency.
Disease Entity
Idiopathic retinal vasospasm is a rare, transient functional disorder characterized by episodic constriction of retinal arterioles leading to temporary retinal ischemia.
It is considered a diagnosis of exclusion after ruling out embolic, inflammatory, and structural vascular causes.
The condition is often associated with systemic vasospastic tendencies, such as migraine, Raynaud phenomenon, or other forms of vascular dysregulation.
Unlike permanent vascular occlusive diseases, idiopathic retinal vasospasm does not typically result in structural retinal damage when episodes are brief and infrequent.
The disorder is part of a broader spectrum of vasospastic syndromes affecting ocular and systemic circulation.
Pathophysiology
The pathophysiology of idiopathic retinal vasospasm involves transient dysregulation of vascular tone in retinal arterioles.
Retinal blood flow is normally tightly regulated by autoregulatory mechanisms involving endothelial cells, smooth muscle, and local metabolic factors.
In vasospastic conditions, this balance is disrupted, leading to inappropriate vasoconstriction.
Potential mechanisms include:
- Increased vascular smooth muscle sensitivity to vasoconstrictors
- Endothelial dysfunction with impaired nitric oxide production
- Enhanced sympathetic nervous system activity
- Imbalance between vasodilatory and vasoconstrictive mediators
In susceptible individuals, triggers such as stress, cold exposure, or hormonal fluctuations may precipitate episodes.
Transient vasoconstriction reduces retinal perfusion, resulting in temporary visual symptoms. If prolonged, repeated episodes may theoretically lead to ischemic injury, although this is uncommon in idiopathic cases.
Epidemiology
Idiopathic retinal vasospasm is uncommon and likely underdiagnosed due to its transient nature.
It most frequently affects young to middle-aged adults, with a higher prevalence in women. Many patients have a history of systemic vasospastic disorders, including:
- Migraine
- Raynaud phenomenon
- Low systemic blood pressure
There is no clear racial predilection. Because symptoms are episodic and often resolve spontaneously, many cases may go unreported.
Clinical Features
The hallmark of idiopathic retinal vasospasm is transient monocular visual disturbance.
Typical symptoms include:
- Sudden, temporary vision loss or blurring
- Scotomas
- Shimmering or flickering lights
- Visual dimming
Episodes usually last from seconds to minutes and resolve completely.
Symptoms are often unilateral but may alternate between eyes. Triggers may include:
- Cold exposure
- Emotional stress
- Physical exertion
Importantly, patients are asymptomatic between episodes, and visual acuity is typically normal.
Examination Findings
Between episodes, ophthalmic examination is usually normal.
During an episode, findings may include:
- Segmental or diffuse narrowing of retinal arterioles
- Reduced blood column visibility
- Occasionally, mild retinal pallor in affected areas
Fluorescein Angiography (FA)
FA performed during or shortly after an episode may show:
- Delayed arterial filling
- Segmental perfusion defects
- Absence of embolic material
- No significant leakage
Optical Coherence Tomography (OCT)
OCT is typically normal in transient cases. In rare prolonged episodes, mild inner retinal changes may be observed.
Optical Coherence Tomography Angiography (OCTA)
- Transient reduction in capillary perfusion
- Normalization after resolution
Visual Field Testing
- Transient scotomas corresponding to areas of vasospasm
Because episodes are short-lived, capturing findings during an attack can be challenging.
Differential Diagnosis
Idiopathic retinal vasospasm must be distinguished from other causes of transient or permanent retinal ischemia.
Key differential diagnoses include:
- Amaurosis fugax due to embolic disease
- Branch retinal artery occlusion (BRAO)
- Ocular migraine
- Giant cell arteritis
- Retinal vasculitis
Amaurosis fugax typically results from embolic phenomena and is associated with carotid or cardiac disease.
Branch retinal artery occlusion leads to persistent visual field defects and visible retinal whitening.
Ocular migraine may present with visual aura but often includes bilateral symptoms and cortical features.
Giant cell arteritis should be considered in older patients with systemic symptoms.
A thorough systemic evaluation is essential to exclude serious vascular or inflammatory causes.
Diagnosis
Idiopathic retinal vasospasm is a diagnosis of exclusion.
Key diagnostic criteria include:
- Recurrent transient monocular visual symptoms
- Evidence of retinal vasoconstriction during episodes (if observed)
- Normal examination between episodes
- Absence of embolic, inflammatory, or structural vascular disease
- Negative systemic workup
Investigations may include:
- Carotid Doppler ultrasound
- Cardiac evaluation
- Blood tests for inflammatory and autoimmune conditions
Fluorescein angiography during symptoms can support the diagnosis, but it is not always feasible.
Management
Management focuses on reducing the frequency and severity of vasospastic episodes.
Lifestyle Modification
- Avoidance of triggers such as cold exposure
- Stress management
- Smoking cessation
Pharmacologic Therapy
Calcium channel blockers (e.g., nifedipine, verapamil) are commonly used and may reduce vasospastic episodes.
Other options may include:
- Magnesium supplementation
- Vasodilators
Monitoring
Patients should be monitored for:
- Frequency and severity of episodes
- Development of permanent visual deficits
Referral to neurology or cardiology may be appropriate in selected cases.
Prognosis
The prognosis of idiopathic retinal vasospasm is generally favorable.
Most patients experience transient symptoms without permanent visual impairment.
However, frequent or prolonged episodes may theoretically increase the risk of retinal ischemic damage, although this is uncommon.
With appropriate management, symptom control is often achievable.
Would you have interest in taking retinal images with your smartphone?
Fundus photography is superior to fundus analysis as it enables intraocular pathologies to be photo-captured and encrypted information to be shared with colleagues and patients.
Recent technologies allow smartphone-based attachments and integrated lens adaptors to transform the smartphone into a portable fundus camera and Retinal imaging by smartphone.
RETINAL IMAGING BY YOUR SMARTPHONE
References
- American Academy of Ophthalmology. Basic and Clinical Science Course (BCSC): Retina and Vitreous. San Francisco, CA: AAO; latest edition.
- Yanoff M, Duker JS. Ophthalmology. 5th ed. Elsevier; 2019.
- Flammer J, Konieczka K. The primary vascular dysregulation syndrome: implications for eye diseases. EPMA J. 2017;8(3):209–217.
- Hayreh SS. Transient visual loss. Prog Retin Eye Res. 2011;30(5):359–394.
- Pache M, Flammer J. A sick eye in a sick body? Systemic findings in patients with primary vascular dysregulation. Surv Ophthalmol. 2006;51(2):179–185.
- Riva CE, Logean E, Falsini B. Visually evoked hemodynamic response and neurovascular coupling in the optic nerve and retina. Prog Retin Eye Res. 2005;24(2):183–215.

{kind=link}