
Case Study
A 34-year-old patient presented with a long-standing history of gradual bilateral visual blurring and increasing glare, especially in bright light conditions.

The symptoms had progressed slowly over several years and were not associated with pain, redness, or photophobia. There was a positive family history of similar visual problems in first-degree relatives.
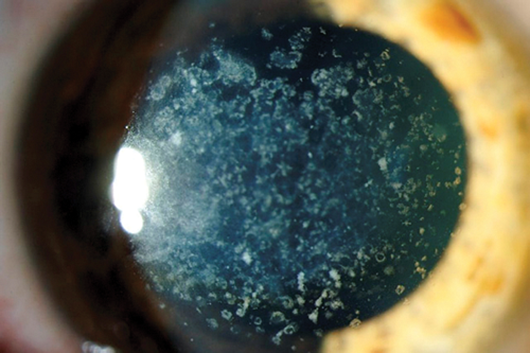
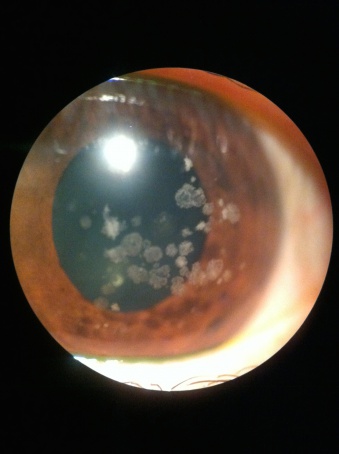
Best-corrected visual acuity measured 20/40 in both eyes. Slit-lamp examination revealed bilateral, symmetric, whitish-gray opacities located predominantly within the corneal stroma, with clear epithelium and endothelium.
The corneal findings were non-inflammatory and showed sharp demarcation from surrounding clear tissue.
Based on clinical features, family history, and characteristic slit-lamp findings, a diagnosis of corneal stromal dystrophy was established.
Disease Entity
Corneal stromal dystrophies are a group of inherited, bilateral, non-inflammatory corneal disorders characterized by abnormal deposition of material within the corneal stroma.
These dystrophies typically present symmetrically, progress slowly, and are not associated with systemic disease. Visual impairment results from progressive stromal opacification and irregularity, rather than active inflammation.
Corneal stromal dystrophies are genetically determined and usually inherited in an autosomal dominant or autosomal recessive pattern.
They often manifest in the first or second decade of life, although symptoms may not become visually significant until adulthood.
Despite their varied histopathologic features, these dystrophies share common clinical characteristics, including clear corneal epithelium and endothelium in early stages.
Pathophysiology
The underlying pathophysiology of corneal stromal dystrophy involves abnormal synthesis, accumulation, or degradation of stromal components such as collagen, glycosaminoglycans, lipids, or amyloid material.
Genetic mutations alter keratocyte function, leading to progressive deposition of abnormal substances within the corneal stroma.
These deposits disrupt the highly organized collagen lamellae that are essential for corneal transparency.
As stromal clarity decreases, light scattering increases, resulting in glare, reduced contrast sensitivity, and gradual visual decline.
In advanced stages, stromal thickening and irregularity may further impair visual acuity.
Classification of Corneal Stromal Dystrophies
Corneal stromal dystrophies include several distinct entities, each with unique clinical and histological features:
-
Granular Corneal Dystrophy: Characterized by discrete, crumb-like white opacities within the stroma.
-
Lattice Corneal Dystrophy: Features include branching, lattice-like amyloid deposits in the stroma.
-
Macular Corneal Dystrophy: Presents with diffuse stromal haze and grayish opacities extending to the peripheral cornea.
-
Avellino Corneal Dystrophy: Displays combined features of granular and lattice dystrophies.
-
Schnyder Corneal Dystrophy: Associated with stromal cholesterol and lipid deposition, sometimes with systemic hyperlipidemia.
Each subtype has a distinct clinical course and impact on vision, although overlap may occur.
Epidemiology
Corneal stromal dystrophies are relatively rare but represent a significant cause of inherited corneal disease worldwide.
The prevalence varies by geographic region and genetic background. Granular and lattice dystrophies are more common in certain populations, while macular dystrophy is more frequently reported in regions with higher rates of consanguinity.
Both sexes are affected equally, and the condition typically presents bilaterally. Symptoms may begin early in life, but visual impairment often becomes more noticeable in adulthood.

Clinical Features
Patients with corneal stromal dystrophy often present with slowly progressive visual symptoms. Common features include:
-
Gradual reduction in visual acuity
-
Increased glare and light sensitivity
-
Reduced contrast sensitivity
-
Visual distortion due to stromal irregularity
-
Typically painless and non-inflammatory course
In some subtypes, recurrent corneal erosions may occur, particularly when deposits extend toward the anterior stroma.
Examination Findings
Slit-lamp examination is key to diagnosis and reveals characteristic stromal opacities with preserved epithelial and endothelial layers, especially in early disease. Additional findings may include:
-
Bilateral, symmetric stromal deposits
-
Clear corneal periphery in early stages
-
Progressive stromal haze in advanced disease
-
Normal corneal sensation in most cases
Anterior segment optical coherence tomography (AS-OCT) can help localize deposits within the stromal layers and assess disease depth.
Differential Diagnosis
The differential diagnosis of corneal stromal dystrophy includes:
-
Corneal scarring from prior infection or trauma
-
Metabolic corneal deposits
-
Salzmann nodular degeneration
-
Post-inflammatory corneal opacities
-
Drug-induced corneal deposits
A detailed history, bilateral symmetry, family history, and lack of inflammation help distinguish dystrophies from acquired corneal diseases.
Diagnosis
Diagnosis is primarily clinical and based on slit-lamp findings and family history. Ancillary tests may include:
-
Anterior segment OCT to evaluate stromal involvement
-
Corneal topography to assess irregular astigmatism
-
Genetic testing in selected cases for definitive classification
-
Histopathology following keratoplasty, when performed
Management
Management depends on disease severity and visual impact. Early or mild cases often require observation only, with regular follow-up to monitor progression.
Conservative Management
-
Optical correction with glasses or contact lenses
-
Lubrication for associated surface symptoms
-
Management of recurrent erosions when present
Surgical Management
-
Phototherapeutic Keratectomy (PTK): Effective for superficial stromal deposits
-
Deep Anterior Lamellar Keratoplasty (DALK): Preferred when deeper stromal involvement is present with a healthy endothelium
-
Penetrating Keratoplasty (PK): Reserved for advanced cases with full-thickness involvement
Recurrence of dystrophy in graft tissue is possible, particularly in granular and lattice dystrophies, and long-term follow-up is essential.
Prognosis
The visual prognosis varies depending on the subtype and severity. Many patients maintain useful vision for years with conservative management.
Surgical outcomes are generally favorable, although recurrence can affect long-term graft clarity. Early diagnosis and appropriate intervention help preserve vision and improve quality of life.
Prevention and Genetic Counseling
There is no known method to prevent corneal stromal dystrophy. However, genetic counseling is recommended for affected individuals and families, especially in autosomal dominant forms.
Early screening of family members allows timely diagnosis and monitoring.
Conclusion
Corneal stromal dystrophy represents a diverse group of inherited corneal disorders characterized by progressive stromal deposition and gradual visual decline.
Accurate diagnosis, careful monitoring, and tailored management strategies are essential for optimizing visual outcomes.
Advances in imaging and surgical techniques continue to improve the prognosis for patients affected by these visually significant corneal conditions.
HOW TO TAKE SLIT-LAMP EXAM IMAGES WITH A SMARTPHONE?
Smartphone slit-lamp photography is the new advancement in the field of science and technology in which photographs of the desired slit-lamp finding can be taken with smartphones by using the slit-lamp adapters.
Slit-lamp Smartphone photography
References
-
Weiss JS, Møller HU, Aldave AJ, et al. IC3D classification of corneal dystrophies—Edition 2. Cornea.
-
Klintworth GK. Corneal dystrophies. Orphanet Journal of Rare Diseases.
-
Aldave AJ, Sonmez B, Bourla N. Corneal dystrophies in the molecular era. American Journal of Ophthalmology.
-
Krachmer JH, Mannis MJ, Holland EJ. Cornea. Elsevier.
-
Waring GO, Rodrigues MM, Laibson PR. Corneal dystrophies: Clinical, pathologic, and genetic features. Survey of Ophthalmology.

{kind=link}