
Case Study
A 67-year-old woman underwent uncomplicated cataract surgery with intraocular lens implantation.

The immediate postoperative period was smooth, but by day 10, she returned with complaints of worsening vision, increasing floaters, and mild ocular discomfort.
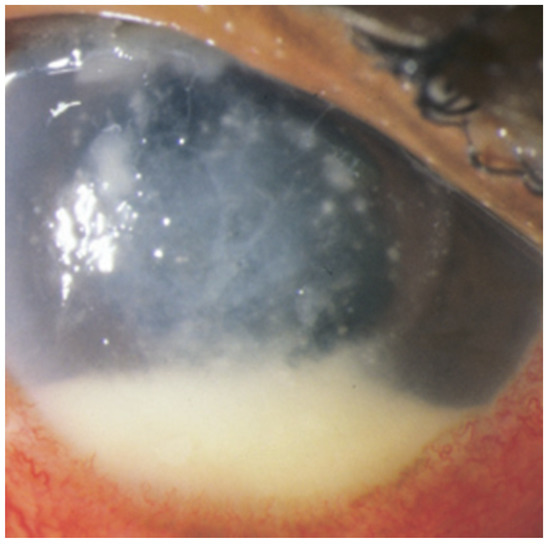
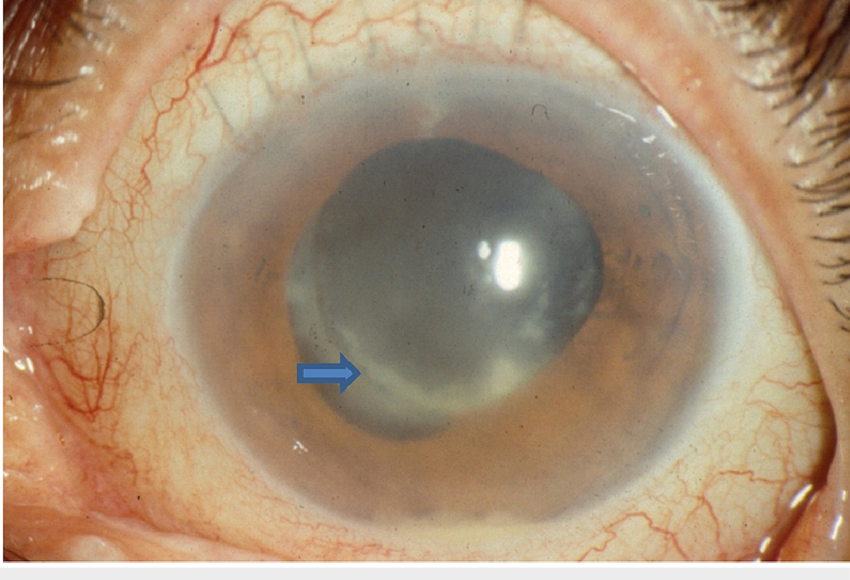
Visual acuity had dropped from 20/40 on day 1 to counting fingers. Slit-lamp examination revealed an anterior chamber reaction with a mild hypopyon and fluffy, white clumps adhering to the posterior capsule.
Fundus view was hazy, but B-scan ultrasonography showed dense vitreous opacities with membranous strands.
Given the subacute presentation and characteristic “cotton-ball” vitreous lesions, postoperative fungal endophthalmitis was strongly suspected.
Aqueous and vitreous taps were performed and cultured. Intravitreal voriconazole was injected empirically, followed by early pars plana vitrectomy.
Cultures later confirmed Candida parapsilosis. After a prolonged course of intraocular and systemic antifungal therapy, the patient’s intraocular inflammation resolved, but final visual acuity stabilized at 20/80.
Disease Entity
Postoperative Fungal Endophthalmitis is a sight-threatening intraocular infection caused by fungal pathogens that enter the eye during or shortly after intraocular surgery, most commonly cataract extraction.
Unlike bacterial postoperative endophthalmitis, the fungal form is characterized by an insidious, delayed, and often subtle onset, making early diagnosis challenging.
The disease is most commonly caused by Candida spp., Aspergillus spp., and Fusarium spp.
It is associated with high morbidity and often requires combined systemic, intravitreal, and surgical therapy to prevent irreversible visual loss.
Pathophysiology
Fungal organisms introduced into the eye during surgery can proliferate slowly within the intraocular environment.
Key mechanisms include:
-
Direct inoculation during surgery, often due to contaminated solutions, instruments, intraocular lenses, or the surgical field.
-
Delayed growth due to the slow replication rate of fungi, leading to later presentation.
-
Biofilm formation on intraocular lenses and capsular bag remnants, particularly with Candida species.
-
Chronic granulomatous inflammation, with formation of white plaques, vitreous strands, and “snowball” lesions.
Filamentous fungi such as Aspergillus trigger more aggressive inflammation, often leading to rapid structural destruction of ocular tissues.
Epidemiology
-
Represents 5–10% of postoperative endophthalmitis cases worldwide.
-
More common in tropical and subtropical regions where environmental fungi are prevalent.
-
Candida species predominate in delayed-onset postoperative cases.
-
Occurs more frequently in patients with:
-
Prolonged surgery
-
Diabetes
-
Immunosuppression
-
Surgical wound leaks
-
Use of contaminated intraocular substances (rare but documented)
-
Clinical Features
Postoperative fungal endophthalmitis typically presents 1–4 weeks after surgery, but may appear months later.
Symptoms:
-
Gradual decrease in vision
-
Floaters or cobweb-like shadows
-
Mild to moderate pain (less severe than in bacterial infections)
-
Photophobia
Signs:
Anterior segment:
-
Mild to moderate anterior chamber reaction
-
Small hypopyon (often creamy or fluffy)
-
White plaques on the posterior capsule or the IOL surface
Posterior segment:
-
Vitritis with “string-of-pearls” or “cotton-ball” vitreous opacities
-
Chorioretinitis or focal granulomatous lesions
-
Macular involvement in severe cases
B-scan findings:
-
Dense vitreous opacities with loculated membranes
-
Possible retinal thickening or subretinal abscess in filamentous fungi infections

Differential Diagnosis
-
Delayed-onset bacterial endophthalmitis (e.g., Cutibacterium acnes)
-
Sterile postoperative inflammation
-
Lens-induced uveitis
-
Retained lens material
-
Viral retinitis (rare)
Examination Findings
-
Slit-lamp: granulomatous keratic precipitates, anterior chamber cells, small hypopyon.
-
Fundus exam: vitreous haze, white chorioretinal lesions, plaques on IOL surface.
-
OCT: intraretinal hyperreflective lesions, vitreal inflammatory aggregates.
-
B-scan: dense vitreous opacities if the view is poor.
Diagnosis
Diagnosis relies on clinical suspicion and laboratory analysis.
Diagnostic Tools:
-
Aqueous and vitreous tap for smear, culture, and PCR.
-
PCR-based fungal detection — high sensitivity, rapid turnaround.
-
Fungal cultures — gold standard, but may require days to weeks.
-
Blood cultures if Candida infection is suspected.
-
OCT and fundus imaging for posterior segment evaluation.
Delayed presentation and low organism load often make diagnosis challenging.
Management
Treatment requires a multimodal approach combining intravitreal therapy, systemic antifungals, and surgery when necessary.
1. Intravitreal Antifungal Therapy
-
Voriconazole (100 µg/0.1 mL): broad-spectrum, effective against Candida and Aspergillus.
-
Amphotericin B (5–10 µg/0.1 mL): potent for Candida; risk of retinal toxicity.
Repeated injections may be needed depending on clinical response.
2. Systemic Antifungal Therapy
Indicated in most cases, especially Candida infections.
Common choices:
-
Oral or IV voriconazole
-
Fluconazole (particularly for Candida species)
-
Amphotericin B for refractory cases
Duration: 4–6 weeks or until complete clinical resolution.
3. Pars Plana Vitrectomy (PPV)
Vitrectomy improves outcomes by:
-
Removing infectious load
-
Breaking vitreous membranes
-
Allowing better drug penetration
-
Removing fungal biofilm or plaques
-
Treating complications such as retinal detachment
Early PPV is recommended for patients with severe vitritis or poor visual acuity at presentation.
4. Management of Complications
-
Retinal detachment
-
Macular scarring
-
Chronic uveitis
-
Recurrent infection
These may require additional surgery or prolonged therapy.
Prognosis
Prognosis varies depending on the organism and the timing of therapy.
-
Candida endophthalmitis: moderate outcomes, vision often stabilizes between 20/60–20/200.
-
Aspergillus and Fusarium infections: poorer outcomes with high rates of retinal necrosis.
-
Delayed diagnosis: increases risk of irreversible vision loss.
Early detection and aggressive management significantly improve prognosis.
Prevention and Follow-Up
-
Strict sterilization protocols in the operating room
-
Monitoring for contaminated surgical materials (rare events but critical)
-
Early review of patients with unusual postoperative inflammation
-
Long-term follow-up to monitor for recurrence or complications
HOW TO TAKE SLIT-LAMP EXAM IMAGES WITH A SMARTPHONE?
Smartphone slit-lamp photography is the new advancement in the field of science and technology in which photographs of the desired slit-lamp finding can be taken with smartphones by using the slit-lamp adapters.
Slit-lamp Smartphone photography
References
-
Silva RA, et al. Fungal endophthalmitis after cataract surgery: clinical presentation and outcomes. Ophthalmology.
-
Binder MI, et al. Candida postoperative endophthalmitis: management strategies. Surv Ophthalmol.
-
Gupta A, et al. Fungal infections in ophthalmology – diagnostic and therapeutic advancements. Retina Journal.
-
Ho IV, et al. Outcomes of vitrectomy in postoperative fungal endophthalmitis. Am J Ophthalmol.
Slit-lamp Smartphone photography

RETINAL IMAGING BY YOUR SMARTPHONE
{kind=link}