
Case Study
A 38-year-old male presented with sudden blurred vision and floaters in both eyes for two weeks. He denied ocular trauma or previous eye disease but reported a recent skin rash and malaise.

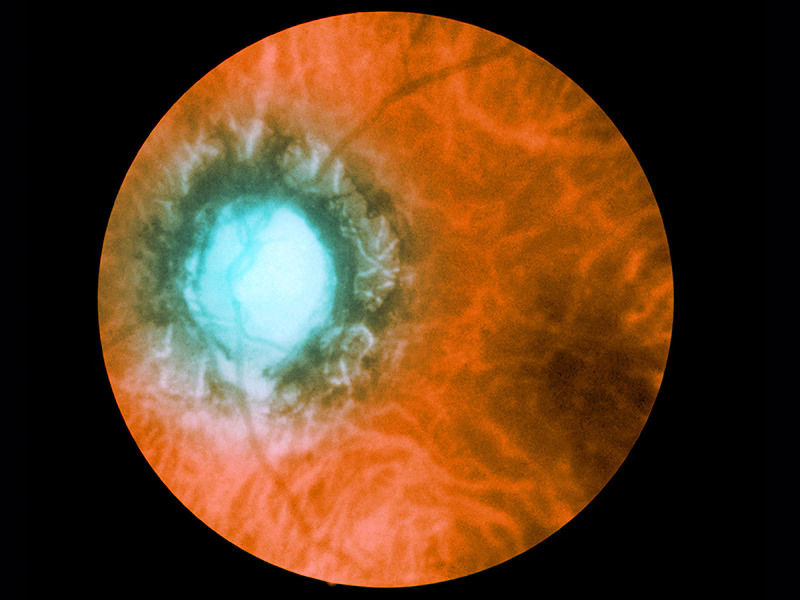
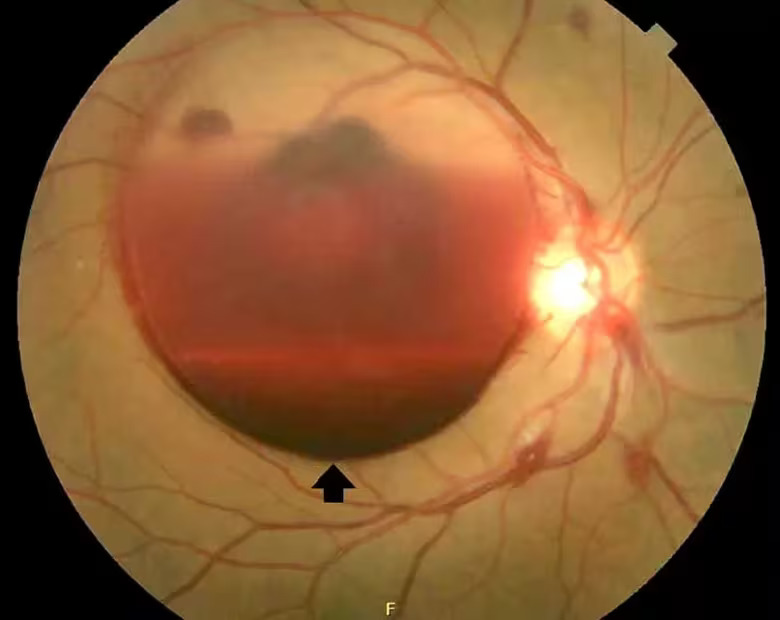
Fundus examination revealed multifocal yellow-white placoid lesions at the posterior pole, vascular sheathing, and mild vitritis.
Fluorescein angiography showed early hypofluorescence with late staining, while optical coherence tomography (OCT) demonstrated disruption of the ellipsoid zone and subretinal fluid.
Serologic testing revealed positive Treponema pallidum particle agglutination (TPPA) and a rapid plasma reagin (RPR) titer of 1:128, confirming the diagnosis of ocular syphilis with posterior uveitis and retinitis.
The patient received intravenous penicillin G for 14 days, leading to gradual visual recovery and resolution of retinal lesions.
Disease Entity
Ocular Syphilis represents a reactivation or dissemination of Treponema pallidum infection involving ocular tissues.
The retina and choroid are common targets, with manifestations ranging from posterior uveitis and retinitis to neuroretinitis, retinal vasculitis, and optic neuritis.
It is often described as “the great imitator” due to its variable presentations that mimic other inflammatory and infectious diseases of the posterior segment.
Pathophysiology
Treponema pallidum, a spirochete bacterium, invades the bloodstream and can affect the eye during any stage of syphilis, though ocular involvement is most frequent during secondary or tertiary stages.
The organism triggers an immune-mediated inflammatory response in ocular tissues, particularly affecting the retinal pigment epithelium (RPE), choroid, and retinal vasculature.
Posterior segment involvement may appear as:
-
Syphilitic placoid chorioretinitis (acute syphilitic posterior placoid chorioretinitis – ASPPC)
-
Diffuse necrotizing retinitis resembling viral retinitis
-
Retinal vasculitis with or without optic disc involvement
-
Neuroretinitis with macular star pattern
Inflammation leads to retinal edema, RPE dysfunction, and serous retinal detachment in severe cases.
In immunocompromised individuals, especially those with HIV co-infection, the infection tends to be more aggressive, bilateral, and recurrent.
Epidemiology
The incidence of ocular syphilis has risen in recent years due to increasing syphilis infections globally, particularly among men who have sex with men (MSM) and individuals co-infected with HIV.
-
Ocular involvement occurs in approximately 1–5% of secondary and tertiary syphilis cases.
-
The mean age of affected patients is between 30–50 years, with a male predominance.
-
Bilateral ocular involvement occurs in up to 40% of cases.
Clinical Features
Ocular syphilis can affect almost any part of the eye, but retinal and choroidal involvement are particularly significant for vision-threatening outcomes.
Posterior Segment Manifestations include:
-
Syphilitic Posterior Placoid Chorioretinitis (ASPPC):
Large, flat, yellowish placoid lesions at the level of the RPE, typically in the macula or posterior pole.
These lesions may be multifocal and bilateral, and patients often present with rapid visual decline. -
Retinitis:
Focal or diffuse whitening of the retina, sometimes mimicking acute retinal necrosis (ARN).
Associated vitritis may obscure the fundus view. -
Retinal Vasculitis:
Involvement of retinal arterioles and venules, with sheathing and perivascular leakage on angiography.
Occlusive vasculitis may cause branch or central retinal vein/artery occlusion. -
Neuroretinitis:
Optic disc edema with a macular star of lipid exudates, occasionally seen in secondary syphilis. -
Chorioretinitis:
Multifocal choroidal lesions with overlying retinal involvement, resembling tuberculosis or sarcoidosis.
Other Ocular Findings:
-
Anterior uveitis (granulomatous or non-granulomatous)
-
Intermediate uveitis
-
Optic neuritis
-
Vitritis
Examination Findings
-
Fundus examination: Yellow-white placoid lesions in macula, vascular sheathing, and disc hyperemia.
-
Fluorescein angiography (FA): Early hypofluorescence with late hyperfluorescent staining, vascular leakage, and disc leakage.
-
Optical Coherence Tomography (OCT): Disruption of outer retinal layers (ellipsoid zone, RPE), hyperreflective deposits at the RPE, and subretinal fluid in ASPPC.
-
Indocyanine Green Angiography (ICGA): Hypofluorescent spots due to choroidal involvement.
Differential Diagnosis
Ocular syphilis can mimic many retinal and choroidal diseases. The main differentials include:
-
Viral retinitis (CMV, HSV, VZV)
-
Toxoplasmosis
-
Tubercular choroiditis
-
Sarcoid uveitis
-
Acute posterior multifocal placoid pigment epitheliopathy (APMPPE)
-
Vogt-Koyanagi-Harada (VKH) disease
Serologic testing is critical to distinguish syphilis from these entities.
Diagnosis
Diagnosis requires a combination of clinical suspicion and laboratory confirmation.
1. Serologic Testing:
-
Treponemal tests: FTA-ABS (Fluorescent Treponemal Antibody Absorption), TPPA (Treponema Pallidum Particle Agglutination).
-
Non-treponemal tests: RPR (Rapid Plasma Reagin) or VDRL (Venereal Disease Research Laboratory) test – used to monitor treatment response.
2. Ocular Imaging:
-
FA and OCT are indispensable for characterizing retinal lesions and monitoring resolution.
3. Systemic Evaluation:
-
Lumbar puncture for cerebrospinal fluid (CSF) analysis should be performed, as ocular syphilis is considered a form of neurosyphilis.
-
HIV testing is mandatory due to frequent co-infection.
Management
1. Medical Therapy:
-
The mainstay of treatment is aqueous crystalline penicillin G 18–24 million units per day intravenously, administered every 4 hours or as continuous infusion for 10–14 days.
-
In penicillin-allergic patients, ceftriaxone 2 g IV daily for 10–14 days is an alternative.
-
Corticosteroids may be added after initiation of antibiotics to control inflammation and minimize a Jarisch-Herxheimer reaction.
-
Follow-up RPR/VDRL titers should be performed at 3, 6, and 12 months to ensure adequate response.
2. Ocular Management:
-
Topical corticosteroids and cycloplegics for anterior segment inflammation.
-
Systemic steroids may be used cautiously for posterior uveitis after initiating antibiotic therapy.
-
Recurrent inflammation warrants reevaluation for treatment failure or reinfection.
3. Management of Complications:
-
Retinal vasculitis leading to occlusion may cause ischemic changes or neovascularization, requiring anti-VEGF therapy or laser photocoagulation.
-
Optic neuropathy requires aggressive systemic treatment to prevent permanent visual loss.

Prognosis
With timely diagnosis and appropriate antibiotic therapy, visual outcomes are generally favorable.
However, delayed treatment may lead to irreversible damage such as optic atrophy, macular scarring, or chronic uveitis.
Patients with HIV co-infection or late-stage disease tend to have poorer outcomes and higher recurrence risk.
Prevention
-
Routine screening for syphilis in high-risk groups.
-
Early treatment of primary and secondary syphilis to prevent dissemination.
-
Patient education regarding symptom recognition and partner notification is crucial for preventing reinfection.
Would you have interest in taking retinal images with your smartphone?
Fundus photography is superior to fundus analysis as it enables intraocular pathologies to be photo-captured and encrypted information to be shared with colleagues and patients.
Recent technologies allow smartphone-based attachments and integrated lens adaptors to transform the smartphone into a portable fundus camera and Retinal imaging by smartphone.
RETINAL IMAGING BY YOUR SMARTPHONE
References
-
Pichi F, et al. “Syphilitic posterior placoid chorioretinitis: a multimodal imaging analysis.” Ophthalmology. 2014;121(11):2348–2359.
-
Aldave AJ, King JA, Cunningham ET Jr. “Ocular syphilis.” Curr Opin Ophthalmol. 2001;12(6):433–441.
-
Hook EW, Marra CM. “Acquired syphilis in adults.” N Engl J Med. 1992;326(16):1060–1069.
-
Mathew RG, Goh BT, Westcott MC. “British Ocular Syphilis Study (BOSS): clinical features and treatment outcomes.” Eye (Lond). 2014;28(7):853–862.
-
Kiss S, Damico FM, Young LH. “Ocular manifestations and treatment of syphilis.” Semin Ophthalmol. 2005;20(3):161–167.

{kind=link}