
CASE REPORT
A 5-year-old girl is referred by her pediatrician because her vision screen revealed decreased visual acuity in the left eye. The child’s mother reports that the child is otherwise healthy, was born at full term, and has met all developmental milestones.


However, the left eye occasionally appears to turn inward. The child seems to ignore people when they approach her on the left side, and she was previously more likely to cry when her car seat was positioned behind the driver. Further history indicates that, as a baby, she did not feed well when given a bottle, and that she occasionally snores.
On examination, she has a slightly wide nasal bridge. Her visual acuity is 20/20 in the right eye and 20/800 in the left eye with LEA symbols. On cover testing, she has a poor fixation with the left eye but seems to demonstrate a 6-diopter left esotropia.
There is a trace left afferent pupillary defect. Following cycloplegia with 2.5 % phenylephrine and 1% cyclopentolate eye drops, her retinoscopy is +0.50 in the right eye and -3.00 + 1.50 × 90 in the left eye.
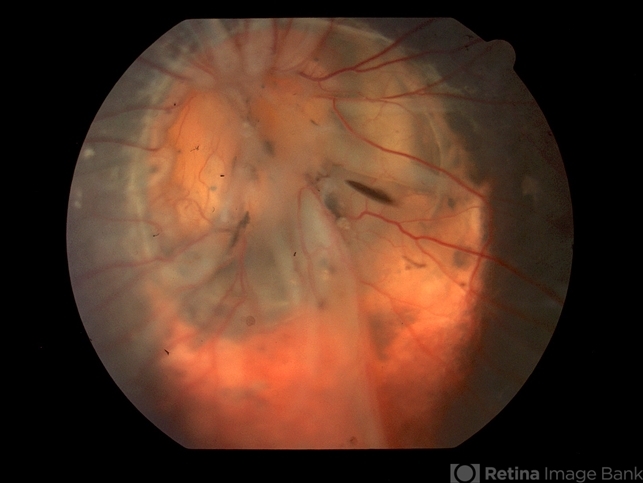
Smartphone fundoscopy reveals a normal-appearing right optic nerve. The left optic nerve is slightly enlarged, with multiple anomalous vessels radiating circumferentially. A tuft of white material obscures the central cup.
There is a wide area of peripapillary pigment abnormality, with zones of hyperpigmentation in clumps, and hypopigmentation. The nerve appears to undulate slightly in and out of focus. The child is diagnosed with morning glory syndrome.
Morning Glory Syndrome: DISEASE entity
Morning Glory syndrome (MGS) is a congenital optic disc pathology. It was first described in 1970 by Kindler. He reported ten cases of congenital optic disc anomaly. The optic nerve head was funnel-shaped.

It had a central whitish fibrous tissue and was surrounded by a ring-shaped area of chorioretinal pigmentary disturbance. The retinal vessels originated as multiple straight narrow branches at the edge of the optic disc.
He called it the morning glory disc because of its resemblance to a morning glory flower. It is a rare sporadic disorder.
Morning Glory Syndrome MANAGEMENT
Early diagnosis and treatment of Morning Glory syndrome (MGS) are essential. The strabismus and anisometropia should be corrected to prevent amblyopia. Full cycloplegic refraction is done, and spectacles are given. Squint may be managed surgically.
Retinal detachment is an associated condition that requires management surgically. Pars plans vitrectomy with or without encircling band is employed. First, a core vitrectomy is done. Then triamcinolone-assisted posterior vitreous detachment is induced.
Meticulous base shaving is done. All breaks are identified and diathermized. If an epiretinal membrane is present, membrane peeling has to be done. Fluid air exchange is done, and subretinal fluid is drained. All breaks are lasered, and a peripheral barrage laser is done.
Silicone oil or gas tamponade is given. Chang et al. and Zhang et al. reported retinal reattachment in all cases with pars plana vitrectomy.

In some cases of retinal detachment, spontaneous attachment has been noticed. Haik et al. reported spontaneous attachment in four patients over seven and a half years. Thus it is important to consider this factor prior to any surgical treatment
Close monitoring of the fellow eye in unilateral cases of MGS is essential. The fellow eye may develop a cataract or retinal detachment. Accordingly, phacoemulsification and lens implantation is done, or vitreoretinal surgery is undertaken.
Would you have interest in taking retina images by smartphone?
Fundus photography is superior to fundus analysis as it enables intraocular pathologies to be photo-captured and encrypted information to be shared with colleagues and patients.
Recent technologies allow smartphone-based attachments and integrated lens adaptors to transform the smartphone into a portable fundus camera and Retinal imaging by smartphone.
RETINAL IMAGING BY YOUR SMARTPHONE
REFERENCES
- Chan RT, Chan HH, Collin HB. Morning glory syndrome. Clin Exp Optom. 2002 Nov;85(6):383-8.
- Kindler P. Morning glory syndrome: unusual congenital optic disk anomaly. Am J Ophthalmol. 1970 Mar;69(3):376-84.
- Harasymowycz P, Chevrette L, Décarie JC, Hanna N, Aroichane M, Jacob JL, Milot J, Homsy M. Morning glory syndrome: clinical, computerized tomographic, and ultrasonographic findings. J Pediatr Ophthalmol Strabismus. 2005 Sep-Oct;42(5):290-5.
- Golnik KC. Cavitary anomalies of the optic disc: neurologic significance. Curr Neurol Neurosci Rep. 2008 Sep;8(5):409-13.
- Fei P, Zhang Q, Li J, Zhao P. Clinical characteristics and treatment of 22 eyes of morning glory syndrome associated with persistent hyperplastic primary vitreous. Br J Ophthalmol. 2013 Oct;97(10):1262-7.
RETINAL IMAGING BY YOUR SMARTPHONE

RETINAL IMAGING BY YOUR SMARTPHONE
{kind=link}