
CASE REPORT
A 74-year-old male patient presented with complaints of decreased vision in the left eye for 3 months, which was gradual in onset and progressive. He had undergone cataract surgery 10 years ago in both eyes, following which he had regained good vision in both eyes.

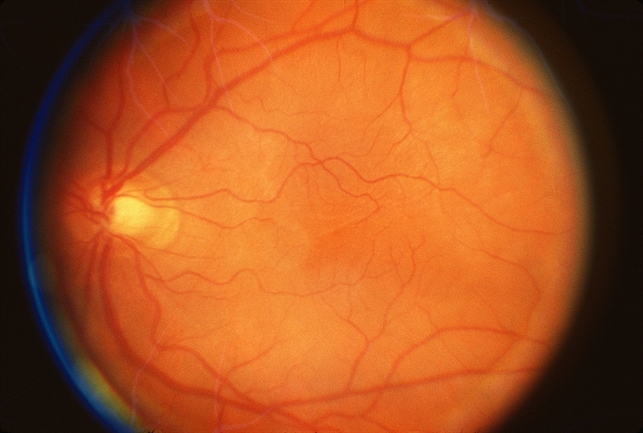
On examination, he was found to have a best corrected visual acuity of 6/9 in the right eye and 6/24 in the left eye. The anterior segment was normal with a well-centered posterior chamber intraocular lens in both eyes. There was no evidence of Posterior capsular opacification.
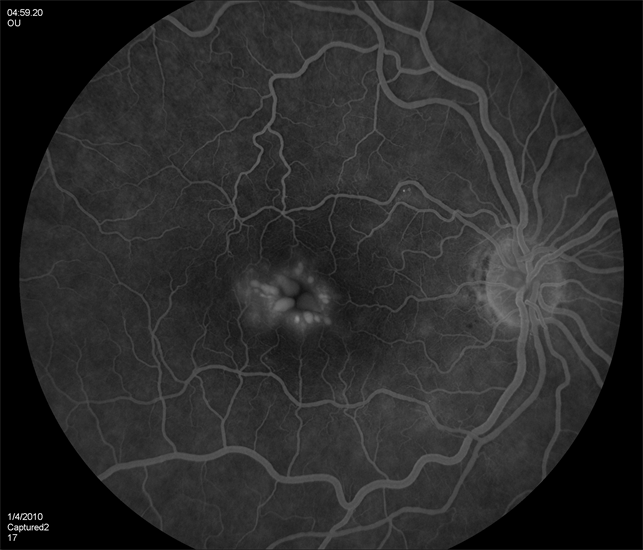
Fundus examination of the left eye was normal except for the absence of a foveal reflex. The Fundus of the right eye was normal. OCT left eye showed characteristic cystoid macular edema and central macular thickness (CMT) was 577 microns. A diagnosis of late-onset cystoid macular edema was made.
Cystoid macular edema disease entity
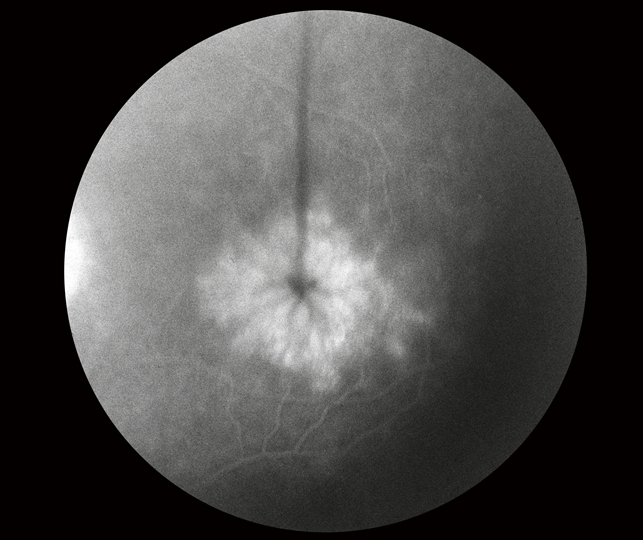
Cystoid macular edema (CME) is a condition that happens when there is a leakage of fluid from the retinal blood vessels into the macula. The accumulation of fluid leads the macula to swell up.
The pathophysiology of cystoid macular edema is based on vasogenic mechanisms. The blood-retinal barrier regulates the passage of ions, proteins, and water flow between retinal vessels and retinal tissues, and inhibits leakage of macromolecules.
The breakdown of the blood-retinal barrier activates components that lead to chemotaxis. Chemotaxis attracts the inflammatory cells to the inflamed tissue and increased vascular hyperpermeability.
This results in the accumulation of fluid in cystoid spaces within the inner layer of the retina especially within the central retina due to its anatomical avascular zone.
Patients with cystoid macular edema have complained of decreased vision due to macular edema, loss of contrast sensitivity and color vision, metamorphopsia (straight lines appear wavy), micropsia difficulty in reading, diplopia, floaters, and central scotoma.
Upon clinical examination, there is significant foveal edema and retinal thickness. Vitritis and optic nerve swelling are also observed.
MANAGEMENT of Cystoid macular edema
Most of the cases of CME are self-limiting and resolve on their own within 3-4 months. However, if CME persists the following medical and surgical treatment should be advised.
- Medical Treatment:
- Topical or Systemically NSAIDs inhibits the activity of cyclooxygenase enzyme that ultimately decreases the production of prostaglandins. NSAIDs have analgesic properties and are considered safe and comfortable. Patients who are at high risk of developing CME after their cataract surgery should receive NSAIDs pre-operatively and post-operatively.
- The intervention of corticosteroid drugs by topically, systemically, or intravitreal inhibits the retinal prostaglandins and leukotrienes synthesis by inhibiting phospholipase activity. Also, they reduce fluid accumulation by decreasing the production of VEGF.
- Carbonic anhydrase inhibitors move the fluid away by stimulating the transport of ions and water from the retina to the choroid.
- Anti-VEGF agents decrease the inflammation in CME by recruitments of leukocytes and increase retinal blood barrier breakdown. By using anti- VEGF there is a marked reduction in fluid accumulation and retinal thickness with a significant improvement in visual acuity with minimal side effects.
- Surgical Treatment: Pars plana vitrectomy can be performed when the macular edema is caused by vitreoretinal tractions and the vitreous is pulling the macula. In PPV the vitreous is removed surgically.
- Laser treatment: Photocoagulation or focal laser eye surgery is used to seal the leaky blood vessels.
Would you have interest in taking retina images by smartphone?
Fundus photography is superior to fundus analysis as it enables intraocular pathologies to be photo-captured and encrypted information to be shared with colleagues and patients.
Recent technologies allow smartphone-based attachments and integrated lens adaptors to transform the smartphone into a portable fundus camera and Retinal imaging by smartphone.
RETINAL IMAGING BY YOUR SMARTPHONE
REFERENCES
- Fung WE. Vitrectomy for chronic aphakic cystoid macular edema. Results of a national, collaborative, prospective, randomized investigation. Ophthalmology. 1985;92:1102–1111.
- Lewis H, Abrams GW, Blumenkranz MS, et al. Vitrectomy for diabetic macular traction and edema associated with posterior hyaloidal traction. Ophthalmology. 1992;99:753-759.
- Pendergast SD, Hassan TS, Williams GA, et al. Vitrectomy for diffuse diabetic macular edema associated with a taut premacular posterior hyaloid. Am J Ophthalmol. 2000;130:178-186.
- Harbour JW, Smiddy WE, Rubsamen PE, et al. Pars plana vitrectomy for chronic pseudophakic cystoid macular edema. Am J Ophthalmol. 1995;120:302-307.
- Stolba U, Binder S, Gruber D, et al. Vitrectomy for persistent diffuse diabetic macular edema. Am J Ophthalmol. 2005;140:295-301.
- Stefaniotou M, Aspiotis M, Kalogeropoulos C, et al. Vitrectomy results for diffuse diabetic macular edema with and without inner limiting membrane removal. Eur J Ophthalmol. 2004;14:137-143.

{kind=link}