
CASE REPORT
A 42-year-old male presented to an ophthalmology department with a history of penetrating injury to the right eye caused by a metallic foreign body one week earlier. The patient underwent primary repair of the corneal laceration and received prophylactic antibiotic therapy.

On examination, his visual acuity in the right eye was counting fingers, and the left eye was 20/20. Slit-lamp examination of the right eye revealed anterior chamber cells, keratic precipitates, and vitreous cells.
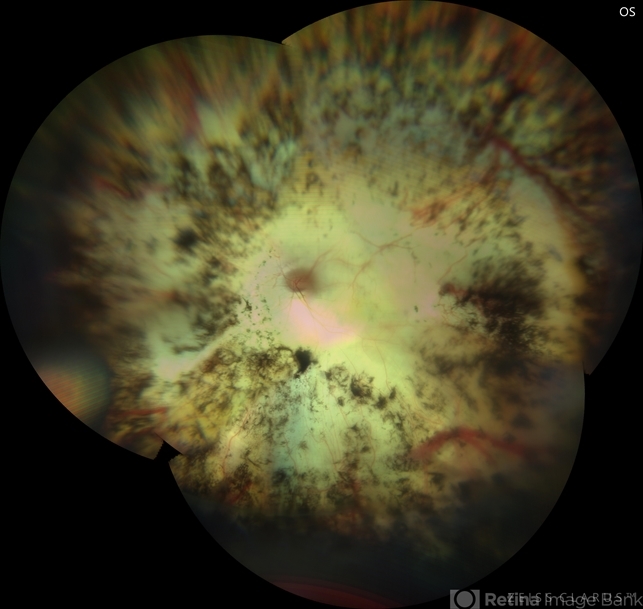
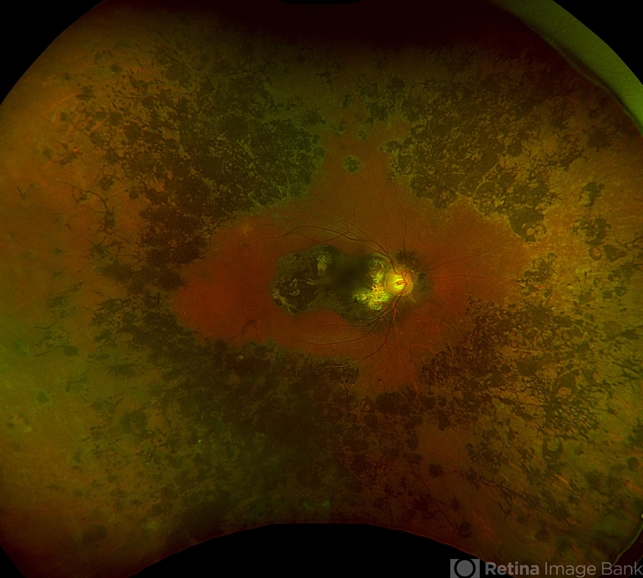
Smartphone Fundoscopy showed optic disc hyperemia and multiple choroidal lesions. The left eye appeared normal. Based on the clinical presentation and history of ocular trauma, a diagnosis of sympathetic ophthalmia was made.
DISEASE
Sympathetic ophthalmia (SO) is a rare, bilateral, granulomatous uveitis caused by exposure of previously immune-privileged ocular antigens from trauma or surgery with a subsequent bilateral autoimmune response to this tissue.

The injured or operated eye is the exciting eye and the contralateral eye is the sympathizing eye. The concept was first described by Hippocrates and the earliest references can be traced back to the 1500s.
It wasn’t until the 1900s that an association with non-trauma-related ocular surgery was published and that a systemic autoimmune etiology was suspected. Several historical figures are hypothesized to have suffered from sympathetic ophthalmia, including Louis Braille, the inventor of modern Braille.
His right eye was injured at the age of 3 when he was playing with a knife, and he subsequently lost vision in both eyes by the age of 5, presumably from sympathetic ophthalmia.
Prior trauma and intraocular surgery are the causes of SO. A growing list of procedures has been associated with this disease and virtually any intraocular event can incite the autoimmune process.
Vitrectomy and cyclo destructive procedures have been associated with potentially higher rates and some authors suggest specifically discussing the risk of sympathetic ophthalmia during informed consent. The interval between the time of injury and the onset of symptoms is variable and has been reported to be from 5 days to 66 years, although the vast majority of cases occur within the first several years.
Due to the rarity of the disease, variable presentation, and potentially long duration between inciting events and the disease process, the epidemiology of sympathetic ophthalmia remains poorly understood.
MANAGEMENT
Corticosteroids are the mainstay of treatment. Steroids should be initiated as soon as the diagnosis is made in the absence of other contraindications and once the infectious workup is negative. In the acute stage, intravenous methylprednisolone pulse therapy reduces the posterior segment changes rapidly.
Along with corticosteroids, immunomodulators such as cyclosporine or azathioprine should be used. SO is one of the few indications where immunomodulatory therapy should be started at the initial presentation only.
Patients should be followed closely and may need to be admitted if they cannot follow up or take the medications as prescribed. Patients should be seen often until they begin to stabilize and improve at which point visits can be spread out.

Prognosis
Sympathetic Ophthalmia is a serious vision-threatening disease. Half of all patients will have 20/40 or worse vision and one-third of all patients will end up legally blind.
However, with modern therapy, there is plenty of hope for patients diagnosed with this disease. Even the exciting eye can have a reasonable visual outcome with prompt and aggressive treatment.
Would you have interest in taking retina images by smartphone?
Fundus photography is superior to fundus analysis as it enables intraocular pathologies to be photo-captured and encrypted information to be shared with colleagues and patients.
Recent technologies allow smartphone-based attachments and integrated lens adaptors to transform the smartphone into a portable fundus camera and Retinal imaging by smartphone.
RETINAL IMAGING BY YOUR SMARTPHONE
REFERENCES
- Albert DM, Diaz-Rohena R. A historical review of sympathetic ophthalmia and its epidemiology. Surv Ophthalmol. 1989;34(1):1-14. doi:10.1016/0039-6257(89)90125-2.
- W Mackenzie. A practical treatise on the diseases of the eye. (ed 3), Longmans, London (1840), pp. 523-534
- Manchester Eye Hospital: Sympathetic Ophthalmia – Complete Loss of Vision-Restoration of Sight by Operative Means. Prov Med J Retrosp Med Sci. 1842 May 28;4(87):155-6.
- Fergus F. Cataract Extraction Followed by Symptoms Suggestive of Sympathetic Ophthalmia. Br Med J. 1923 Feb 3;1(3240):182-3
- RYCHENER RO. Sympathetic ophthalmitis following iridencleisis. Am J Ophthalmol. 1946 Jan;29:96.
RETINAL IMAGING BY YOUR SMARTPHONE

RETINAL IMAGING BY YOUR SMARTPHONE
{kind=link}